
Improving my iron profile
- The tests used to look at iron levels focus on two key proteins (ferritin and transferrin) that form a ‘supply chain’ rather than looking at the blood cells or haemoglobin directly.
- My results show low or barely normal iron levels across the majority of tests.
- If you are iron deficient, it’s important to talk to your doctor and not just take a supplement in case you mask an underlying issue or end up over-compensating and creating an iron excess.
- My issue was a combination of diet (people on a plant-based diet often absorb less iron from their food) and a heavy training programme.
- I opted for a high-quality glycinated iron supplement at 25 mg a day.
- Although improvements in the ‘supply chain’ can be seen quite quickly upon re-test, since blood cells are replaced after around 4 months, it can take a while for that iron increase to show a positive effect on the actual blood cells.
- My 2-month re-test showed a reasonable improvement in iron levels.
- I have maintained the supplement at 25 mg a day and will re-test again in 2 months.
What is the role of iron in the human body?
Iron has an essential role in the transport of oxygen from the lungs to the tissues. Since iron is highly reactive and has an affinity for oxygen, it is used by your blood cells to ‘grab’ oxygen from areas of high oxygen concentration (the lungs) and transport it to regions of lower oxygen concentration (e.g your muscles).
Much of the iron in the body is found in a protein called haemoglobin (strictly speaking, a metalloprotein) which contains four iron ions and each of those ions can grab a single oxygen molecule. Each blood cell in your body contains hundreds of millions of haemoglobin units.
The consequence of low iron levels (and we get into the detail of that in the next section) is reduced oxygen carrying capacity leading to feelings of weakness and fatigue. This can range from being life-threatening though to ‘just’ reduced sporting performance.
Some iron is also found in myoglobin, a protein that stores oxygen specifically in your muscles as a local reservoir.
What were my initial test results (Jan 2026) and what specific measures did it contain?
My iron profile included a number of tests, so I took the time to understand each in a bit more detail.
Iron tests don’t revolve around measurements to do with haemoglobin or red blood cells. Instead, they look at the levels of two key proteins involved in the transport chain leading to the manufacturing of iron rich (hopefully!) haemoglobin for your red blood cells. Those two proteins are:
- Transferrin: Transferrin lives in the plasma and moves iron from the gut (where it has been absorbed from food) to the bone marrow where it hands over its payload of iron to developing red blood cells for the construction of haemoglobin. If there is excess iron for the developing cells (plenty of dietary iron), the transferrin payload is instead transferred to the liver and spleen where it is stored in ferritin (see next) to create a bank.
- Ferritin: Free iron is actually quite toxic and causes oxidative stress in your tissues. Your body handles this by bottling spare iron up inside a shell of a protein called ferritin. Ferritin is stored in your organs (liver, spleen, bone marrow), but a tiny amount leaks into the plasma (the clear liquid that carries the blood cells), and this is what the lab uses for the measurement.
The specific tests involving these proteins are:
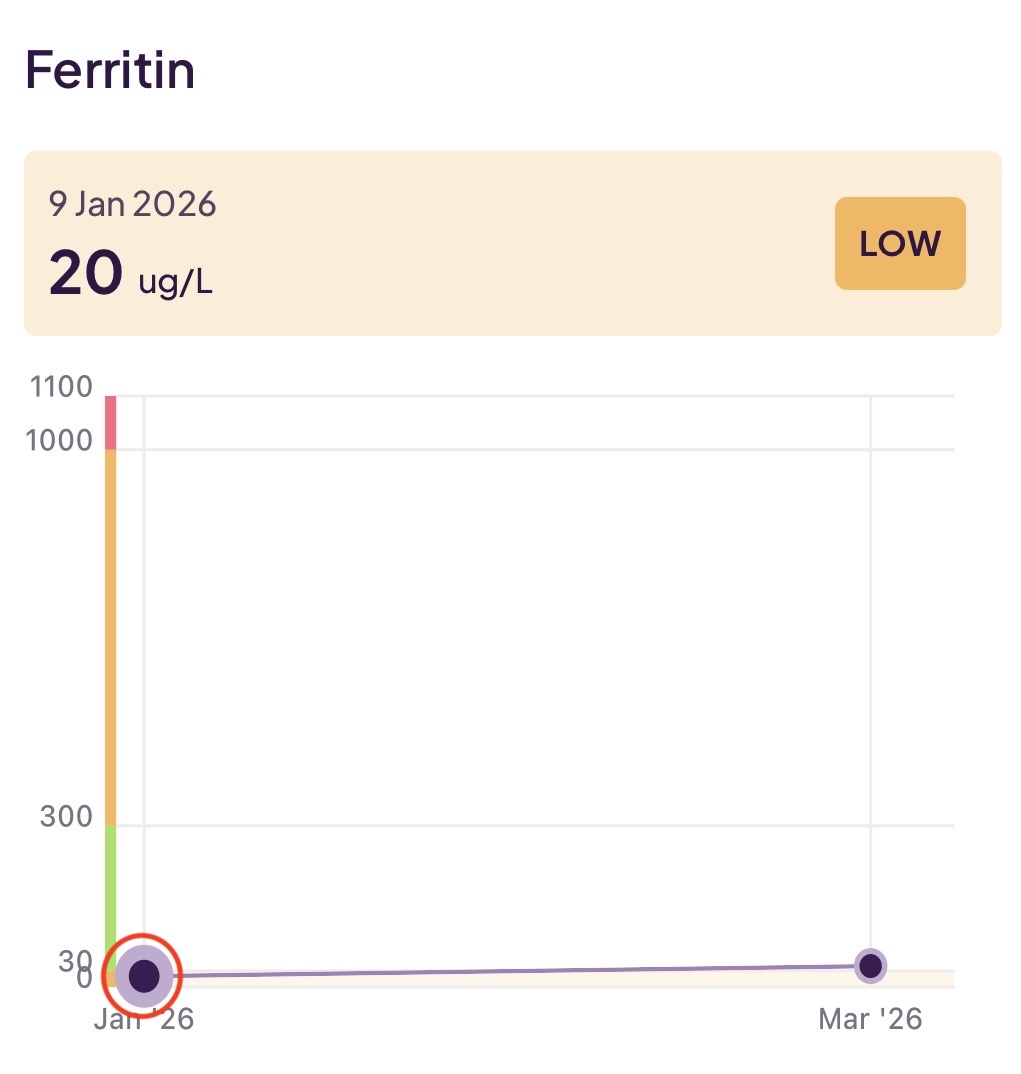
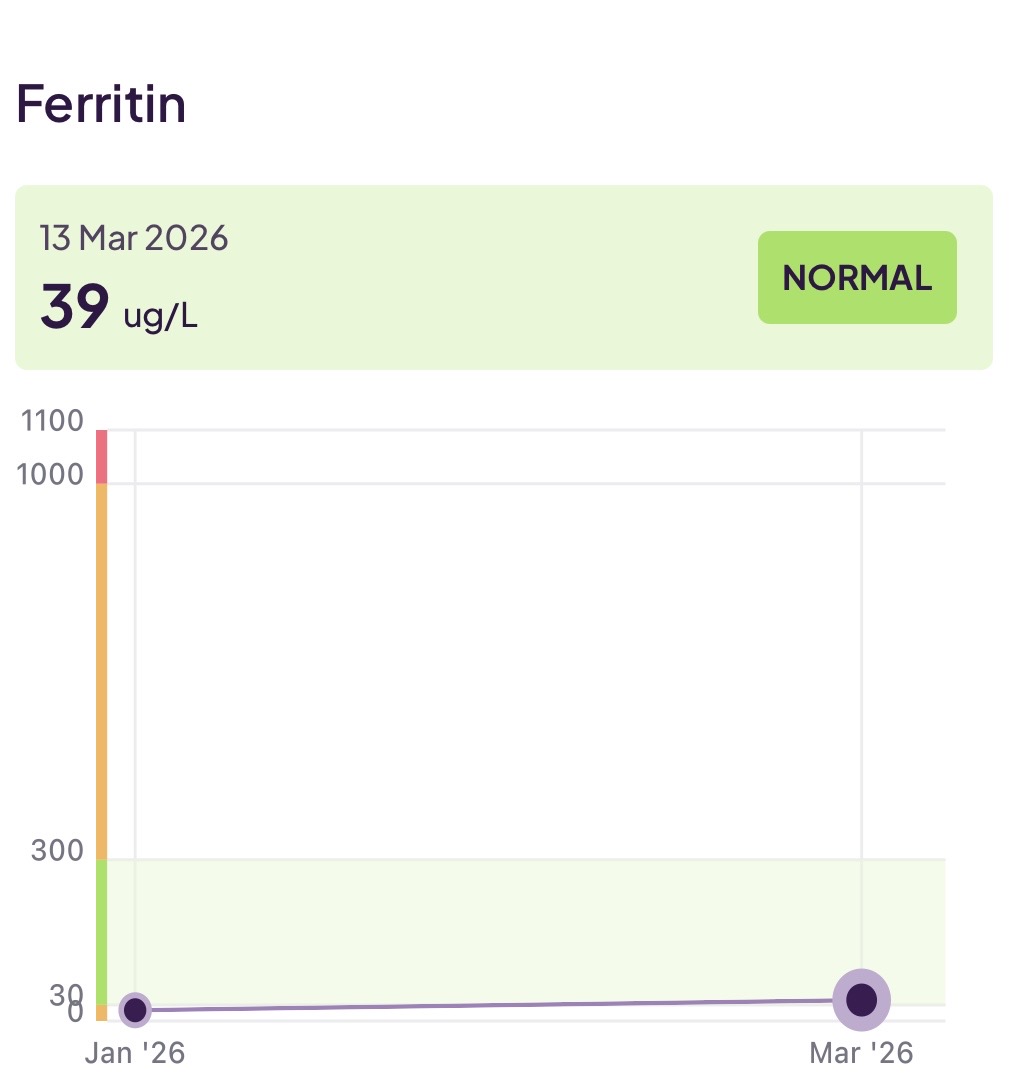
- Ferritin: The ferritin blood test measures the amount of this protein circulating in your blood (as noted above – this is a small amount which has leaked into your plasma from your organs). As your body senses the levels of excess iron coming in from your diet (i.e. beyond what is needed for the manufacturing of haemoglobin), so it scales up and down the production of ferritin and thus the amount of ’leakage’ will go up and down. This test tends to be stable and won’t vary over the duration of a day (e.g. it is not influenced by when you last ate). This reading was abnormal for me at 20 ug/L (just below the normal range of 30–300 ug/L).
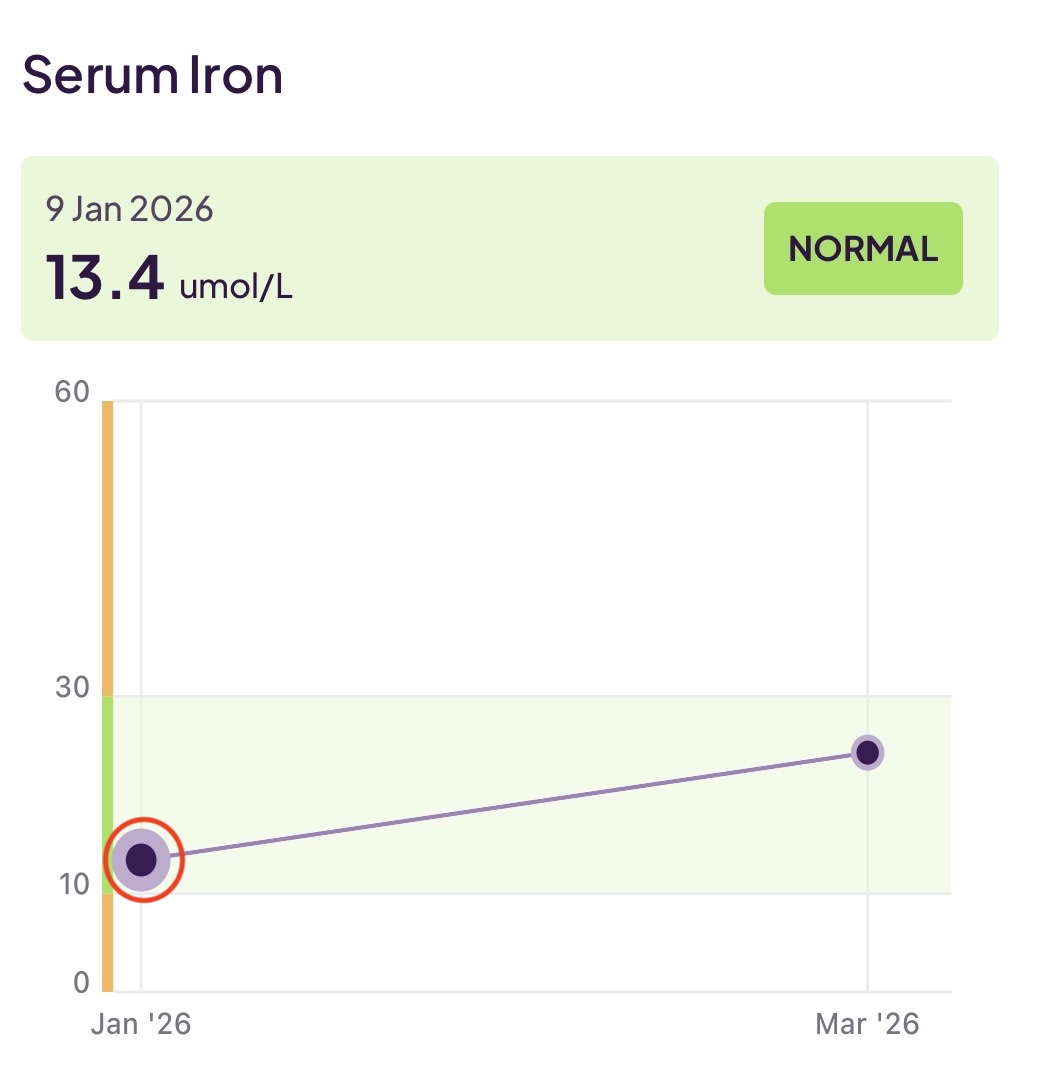
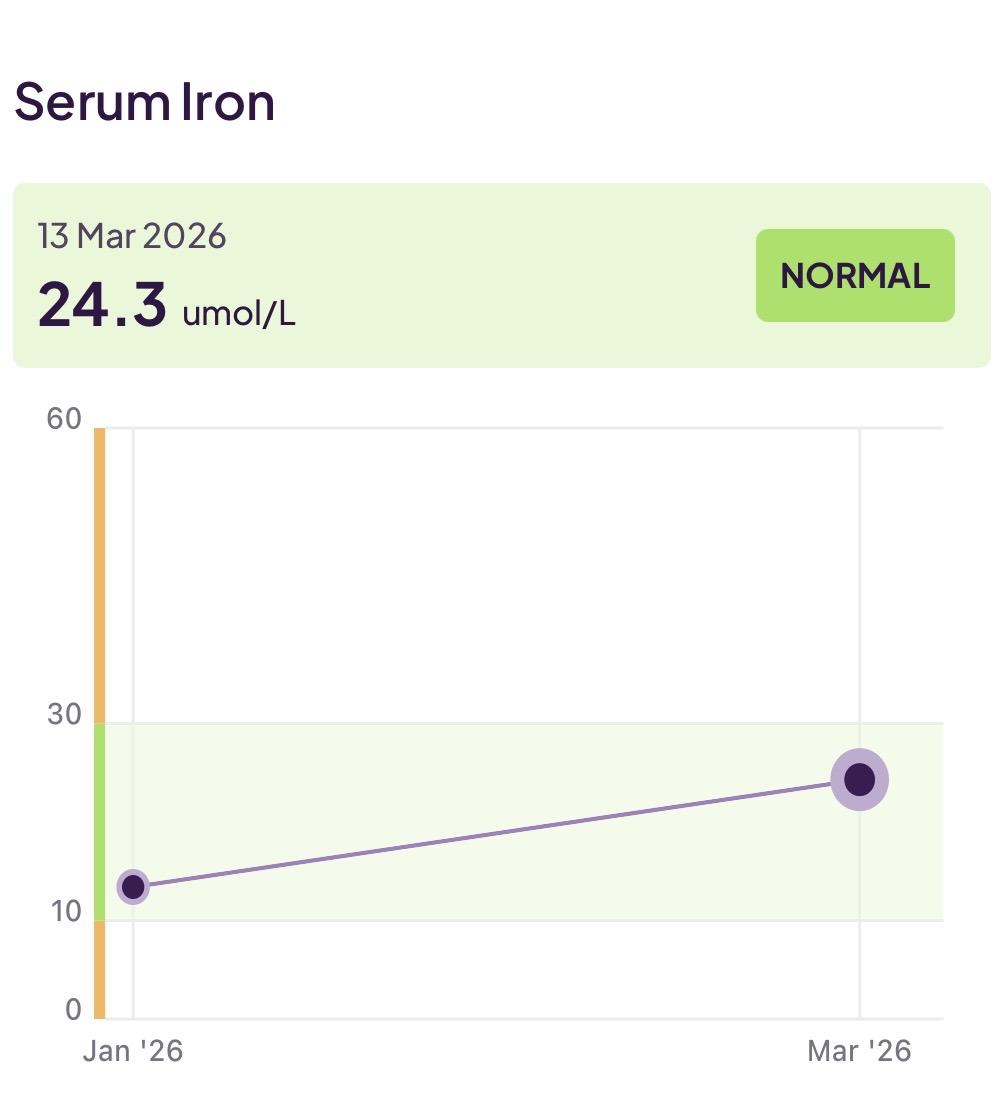
- Serum iron: This is a measure of the amount of iron carried by the transferrin in your blood (strictly, in the plasma) at the moment of the test. If you ate a meal or took an iron supplement close to the blood test, this level can look normal or high even when your ferritin reserves are low. This reading was (just) normal for me at 13.4 umol/L (just into the normal range of 10–30 umol/L).
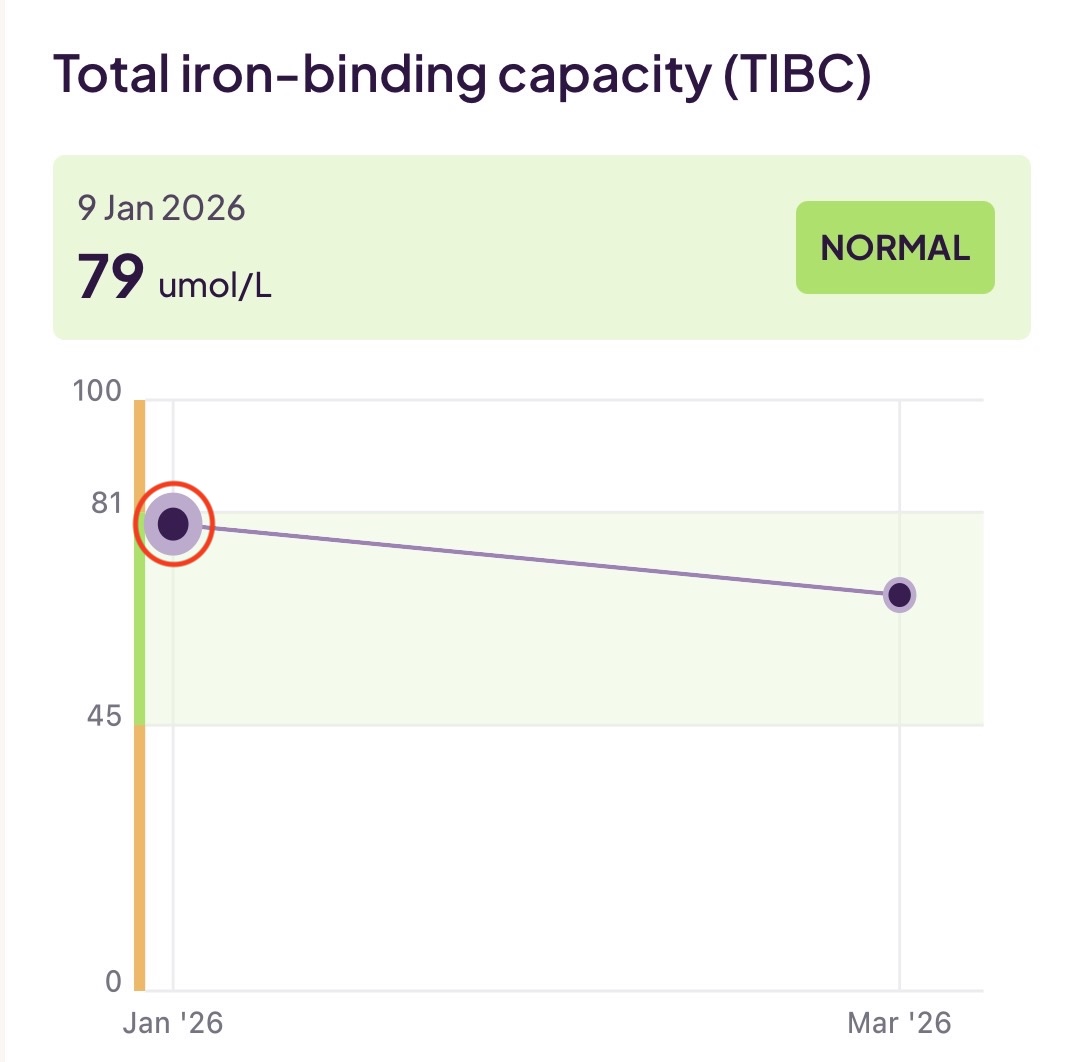
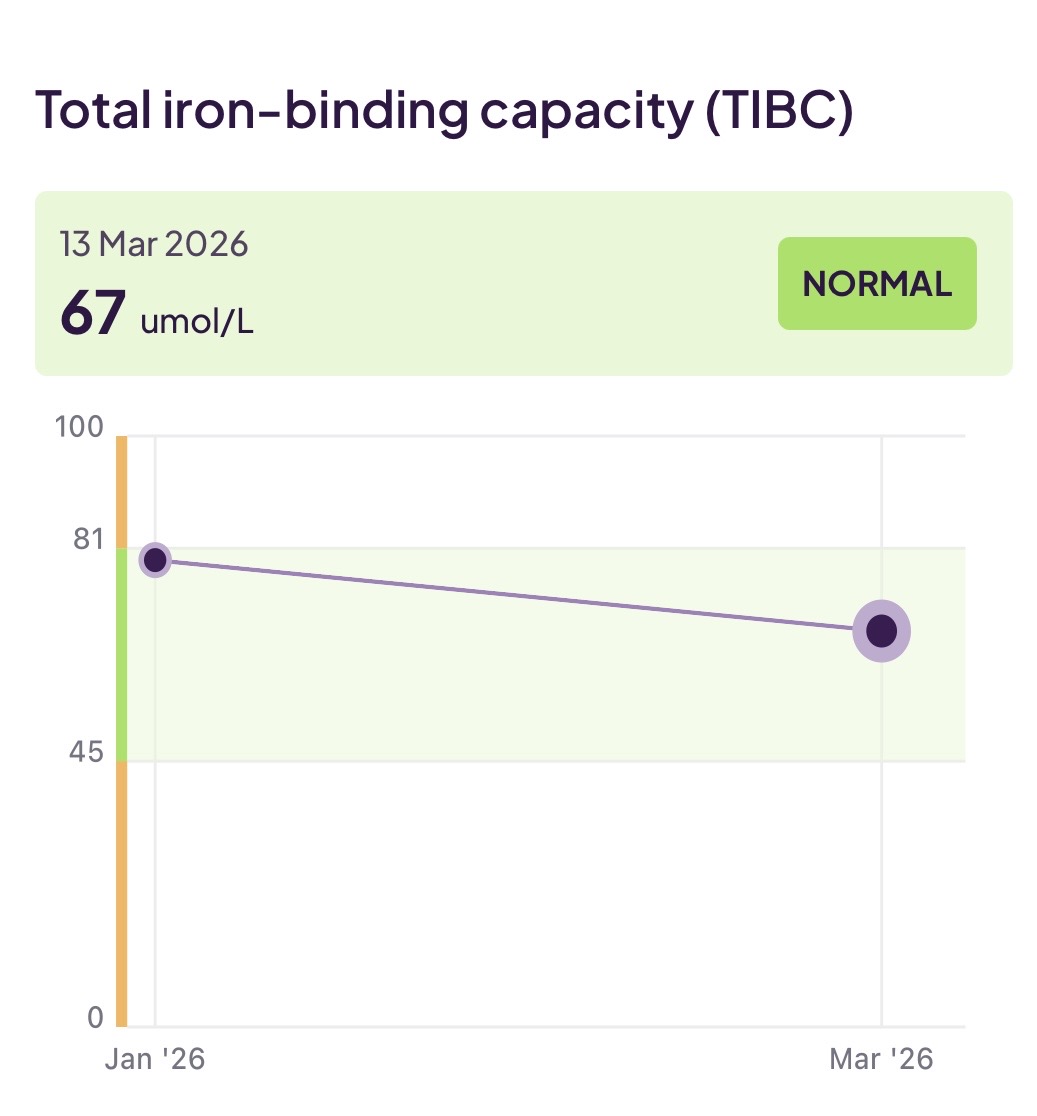
- Total iron-binding capacity (TIBC): This test measures the amount of transferrin circulating in your blood plasma (whereas serum iron - the previous test - measures the actual amount of iron). Thus, the amount of transferrin is a measure of your total capacity to carry iron – but not how much iron is being carried. Counter-intuitively, this will be high when you are iron deficient because if your body senses low iron levels, it will ramp UP the production of transferrin to catch every available atom of iron it can. This reading was normal for me (barely) at 79 umol/L (just into the normal range of 81–54 umol/L).
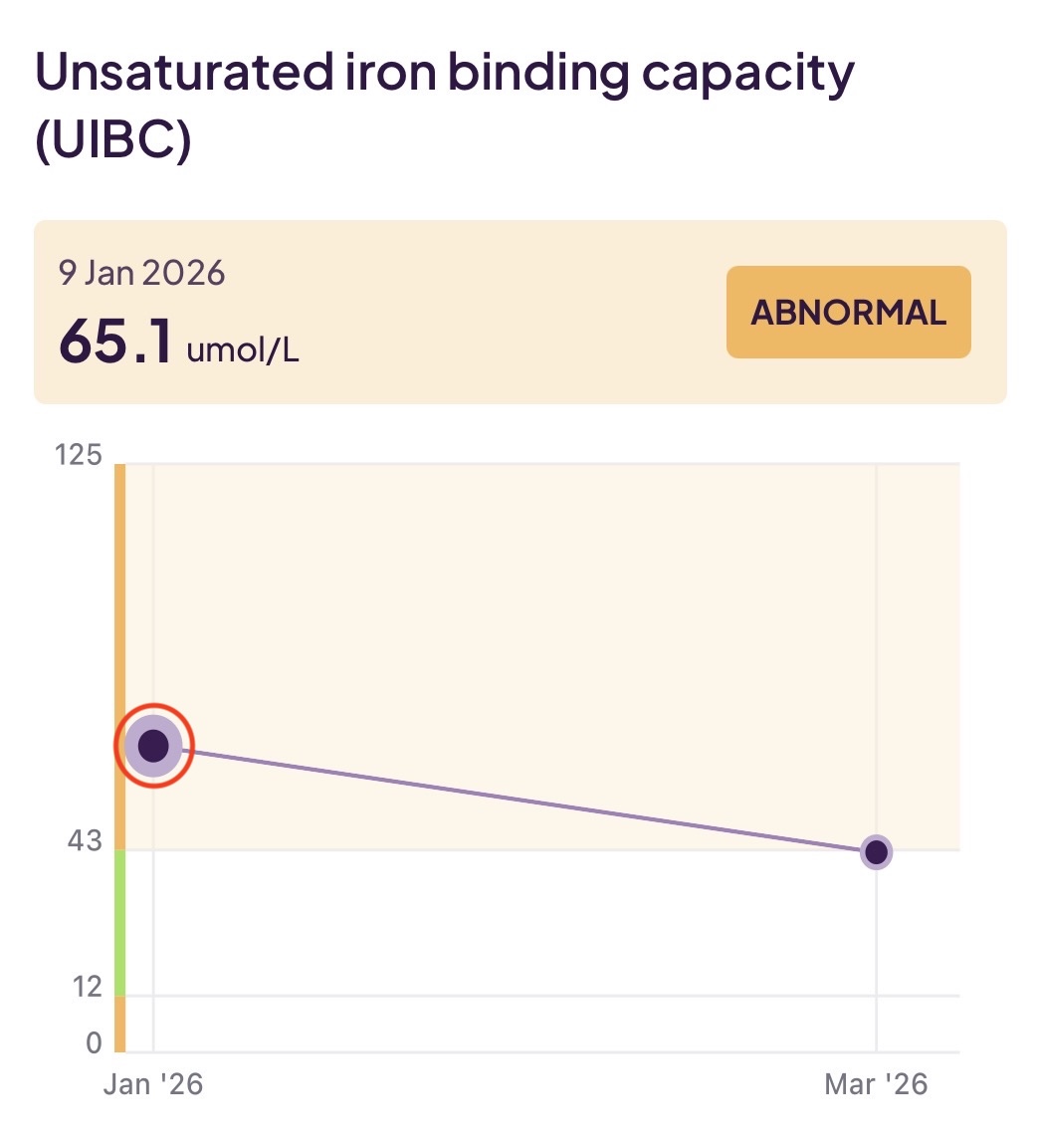
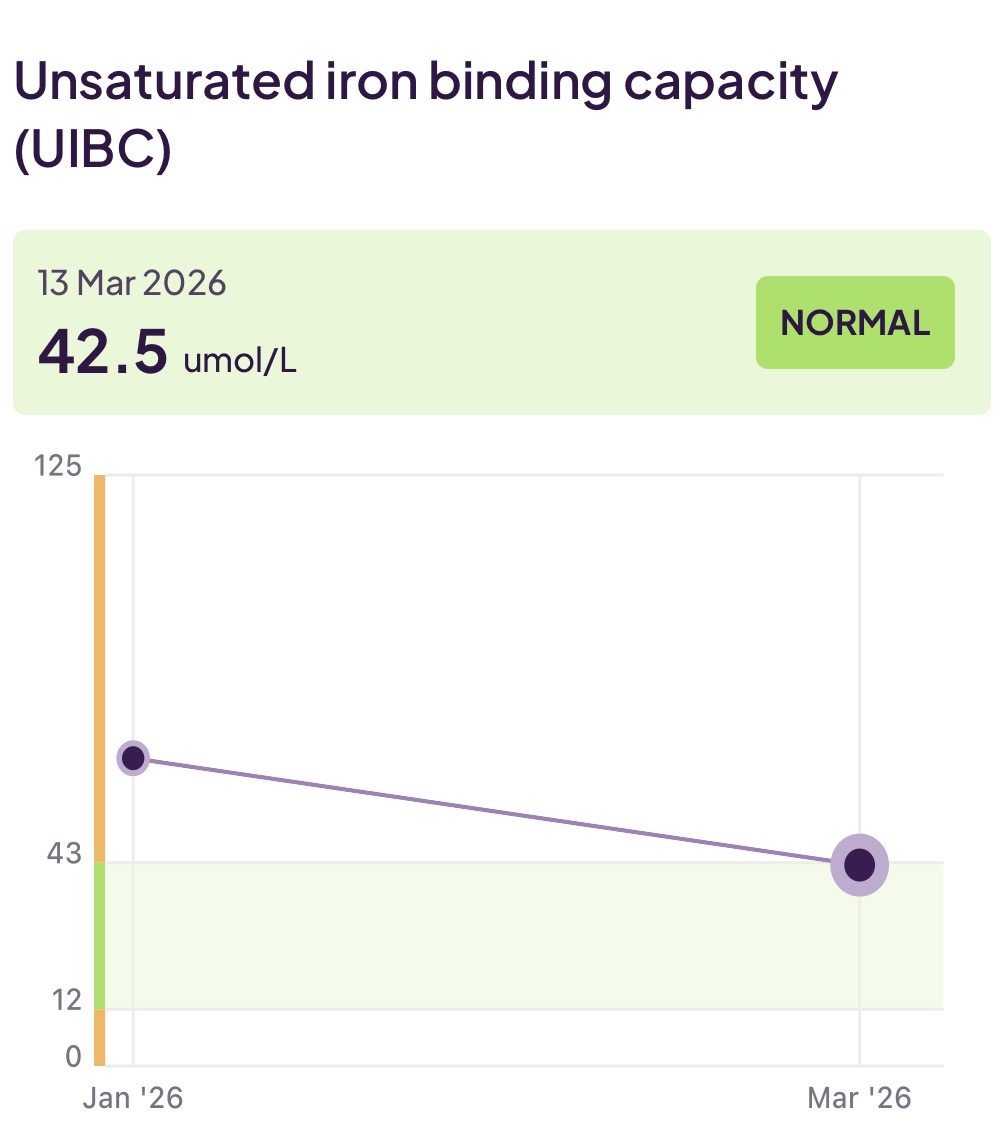
- Unsaturated iron-binding capacity (UIBC): This test measures the amount of transferrin that is not carrying iron. It is a simple calculation of TIBC - serum iron. This measure will be high (out of range) when you are iron deficient. This measure was abnormal for me at 65.1 umol/L well above the normal range of 12–43 umol/L.
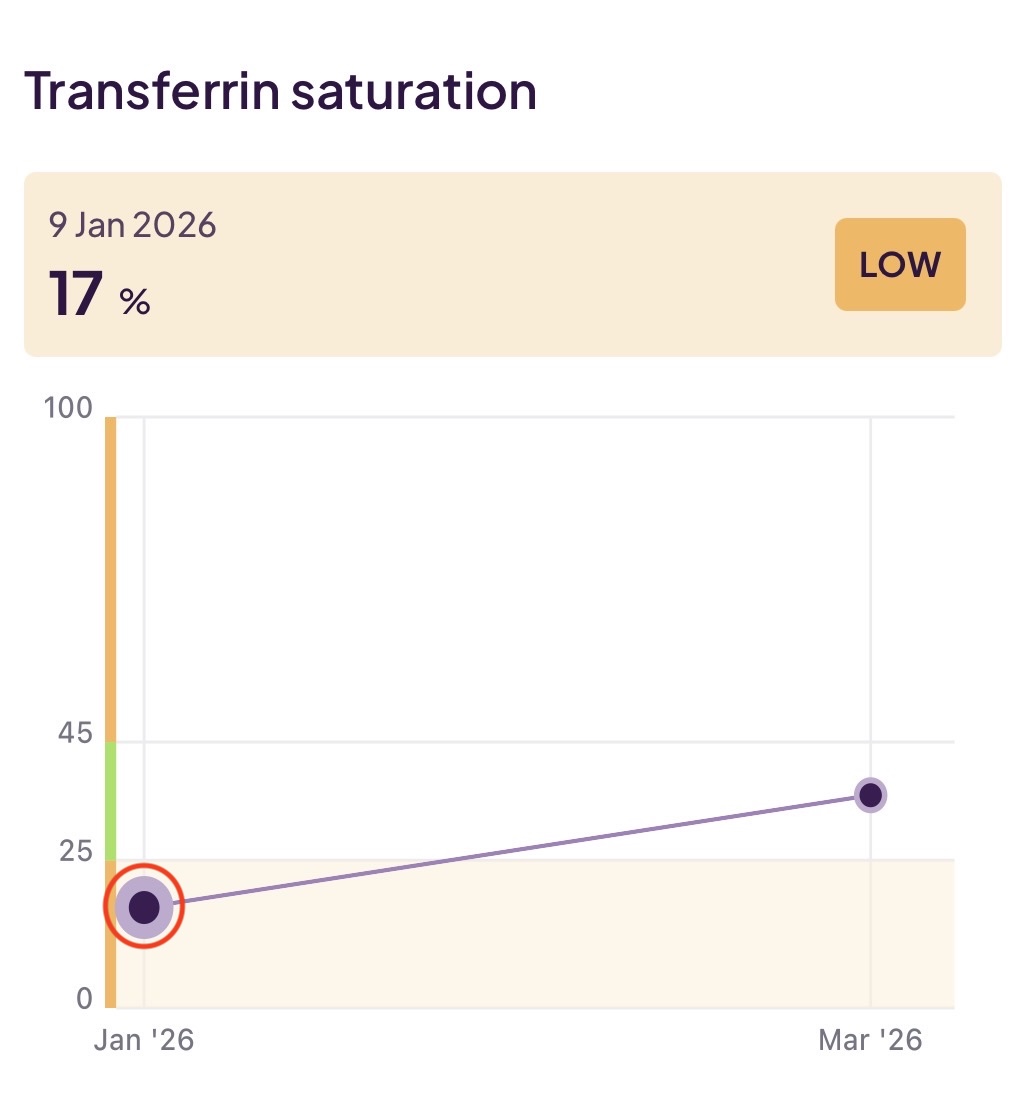
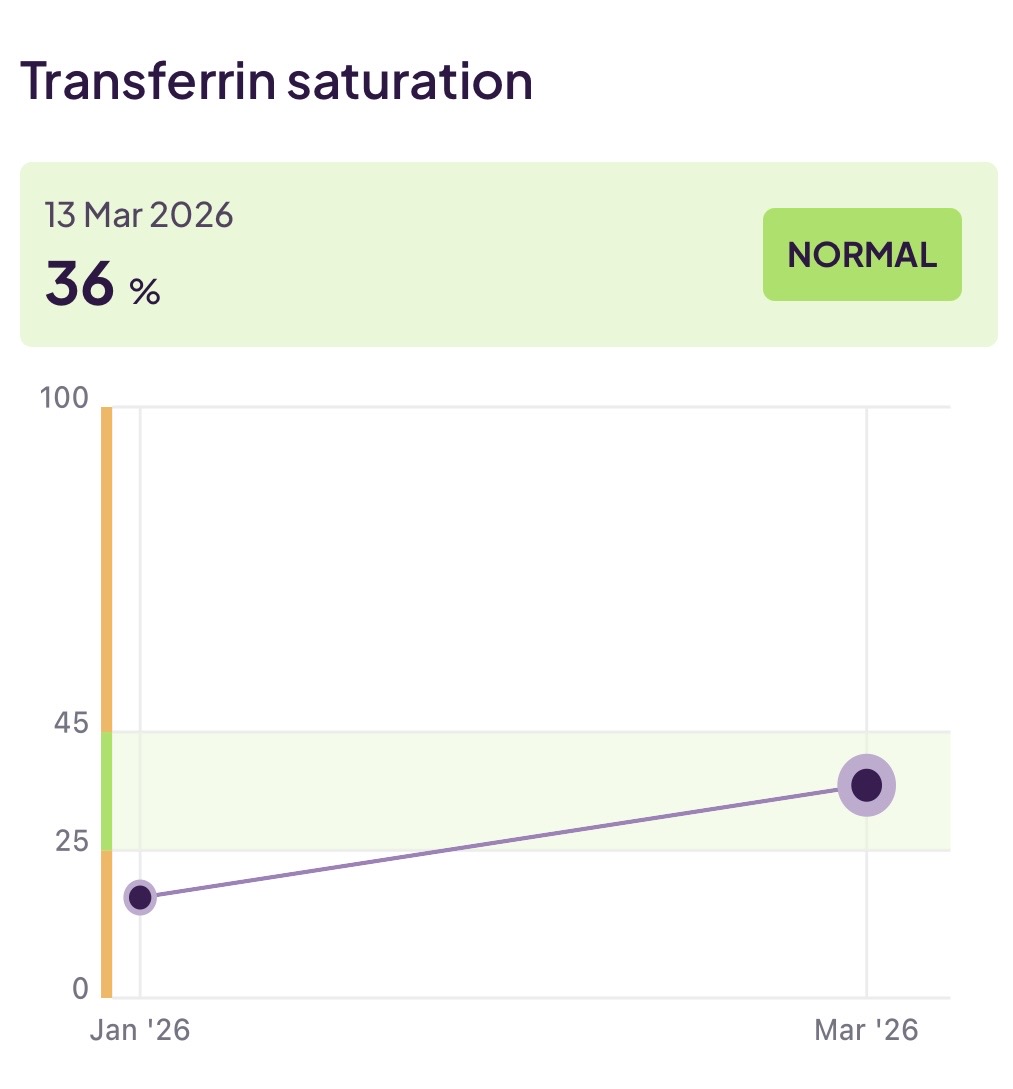
- Transferrin saturation: This test is a simple ratio of your [serum iron]:[total iron binding capacity] expressed as a percentage. It is telling you thus how much iron your transferrin is carrying around. If it was at 30%, that would mean the transferrin is 30% populated. In terms of a simple analogy, if transferrin were a truck, this measure is telling you how many trucks are driving around with a load as opposed to the empty trucks. This reading was abnormal for me at 17% (below the normal range of 25%–45%). This is consistent with being iron deficient. My body has spotted low iron levels and ramped up transferrin production (elevating TIBC)
So, I am definitely seeing an iron deficiency there. The amount of transferrin I have just scrapes into the bottom of the normal range, and the saturation (usage) of that transferrin is only 17% - well below the normal range. Add to that picture below normal levels of ferritin (which is to be expected since there is not much excess iron around for longer term storage) and a demanding training programme I had an issue that needed addressing!
What are some of the possible reasons for iron deficiency?
- Vegetarians and vegans are more prone to low iron levels since plant-based iron is absorbed at a lower rate than meat-based heme-iron.
- Iron uptake can be impacted by consuming tea/coffee at the same time and also dairy produce and grains.
- Endurance sport leads to greater loss of iron through the destruction of blood cells and loss due to heavy sweating.
- In women, loss of blood cells due to your menstrual cycle is a significant factor.
- Internal GI tract issues.
Also, bear in mind that iron (unlike, for example, vitamin C) cannot be easily dumped out by your body and excess supplementation could lead to iron building up in your organs.
Finally, your doctor can also help you work out a good dose to start at to minimise the side effect of iron supplements (such as nausea and constipation).
In my case with a primarily (in fact almost completely) plant-based diet and a heavy training programme, the issue was dietary.
What changes have I made as a result?
I made the following changes:
- Identified and started a high-quality, stomach kind, good-availability iron supplement. As discussed in Big 10 #5 ‘Design Your Personal Supplement Stack Informed by Blood Testing’ I use Iron Bisglycinate from Thorne which it is glycinated (helps with absorption), much kinder to the stomach than ferrous fumarate, and is less vulnerable to caffeine affecting its uptake.
- Identified some good dietary sources of iron. I already consume tempeh and tofu but could easily increase lentils and cooked (that’s an important detail for availability) spinach.
Bear in mind that the response to supplementation won’t be immediate:
- In the first week you can expect serum iron and transferrin saturation to increase – making more iron available for any new red blood cells being created (but having no effect on existing red blood cells).
- After about 6 weeks reserves of ferritin will be rising as your body adjusts to an ongoing, predictable excess of iron that can be sent to storage.
- After about 4 months all of your red blood cells will have been replaced, and you will be feeling the benefits of more capable haemoglobin.
So although early re-tests will let you see improvements in the transport chain, tangible improvements will follow on more slowly behind.
What did my next test show?
I re-tested about 2 months later and will be repeating this again at the 4-month point.
The good news is that now I see:
- A serum iron reading in the middle of the normal range (but bear in mind this could be caused just by having tested closer to a meal/supplements).
- More usefully, a jump in my transferrin saturation to the middle of the normal range.
- Also, more usefully, a drop in TIBC which is a sign of being less iron deficient (see above for the counter-intuitive reason behind this).
- And happily, A slight increase in ferritin into the bottom of the normal range
So, my ‘ready to go’ iron level is now performing well, and the excess is starting to lead to an increase in my ferritin storage. Hopefully, at my next test in another 2 months I will have maintained the transferrin improvements and further increased my ferritin reserves. I see no need to change the level of supplementation at this point (25 mg a day) as I don’t want to risk an iron excess.