

Avoid Ultra-Processed Foods and Control Your Insulin Levels
Use a continuous glucose monitor at home or blood testing from your healthcare provider to identify food and lifestyle choices that are spiking your blood sugar (and thus potentially your insulin levels) so that you can make adjustments to what you eat and the timing of your meals.
Why should you care about insulin and blood glucose?
There is growing evidence that high levels of insulin (hyperinsulinemia) may (along with other factors such as genetics) contribute to elevated risk for all four of our primary threats (cardiovascular disease, neurodegenerative disease, cancer and of course, metabolic disease) due to the inflammatory nature of insulin. There is evidence that what we eat (ultra-processed foods and a diet high in refined sugars) in combination with how frequently we eat leads to hyperinsulinemia and thus exposes us to a whole host of risks (see references below).
Want to look at the science later but, right now, you are just interested in some actions to take?
In an ideal world you’d be able to easily monitor your insulin levels at home. However, at the current point in time that’s a test that you need a health care practitioner to arrange/do for you (which they might well do or have already done if they have concerns). Thus, to get some data yourself easily, you can at least use glucose monitoring as a ‘proxy’ for insulin - on the basis that if your blood glucose is higher than the normal range throughout the day or is showing large spikes you can potentially infer what insulin levels in the blood might also be doing. This is not as valuable or accurate as directly measuring insulin though.
As your blood glucose goes up, then correspondingly behind it, so will your insulin levels go up as your body reacts to process the sugar consumed. Whilst insulin has a vital role to play in your metabolism, it is also an inflammatory hormone with receptors located on the majority of cells in the body. Thus, high long-term levels of insulin (hyperinsulinemia) pose a number of serious health risks:
Metabolic and organ failure: Type 2 Diabetes [1], non-alcoholic fatty liver disease [2], and kidney disease [3].
Cardiovascular damage: Narrowing of the arteries and increased plaque deposits, stiffening of the arteries, and an increased risk of blood clotting leading to an increased risk of heart attacks and strokes. [4]
Neurological damage: Alzheimer’s disease and vascular dementia. [5]
Cancer: An increased risk for some types of cancers. [6]
The growing rise in obesity, insulin resistance, and type 2 diabetes caused by the growth in consumption of ultra-processed foods high in refined carbohydrates is one of the major problems facing 21st century healthcare [7], [8], [9]
What is a Continuous Blood Glucose Monitor (CGM)?
A CGM is a small device that continuously samples your blood to monitor your glucose levels and sends that data to your phone. It enables you to see exactly what is happening to your blood sugar levels minute-by-minute over the day as you eat, train, rest, and sleep. These devices are generally quite discreet, pain-free to fit, and convenient to wear. There are medical/prescription-grade devices used by patients with a diagnosis of diabetes but there are also lifestyle devices that you can purchase over the counter. These are great for people without a diabetes diagnosis but who are interested in their blood sugar levels. The devices are relatively low-cost, disposable, and have a fixed life (although that fixed life does vary device to device). In essence, you are buying the data that the device provides you with rather than the device itself.
Blood glucose science essentials
What does the term ‘sugar’ mean?
Although the word sugar is used as a catch-all term, it can be divided into three specific types:
Glucose: This is found in starchy foods such as bread, pasta, potatoes or in added sugar. This is the body’s primary fuel, and it is the only type of sugar that will trigger a significant insulin response. Excess glucose is stored as a fuel called glycogen in the liver and muscles, and when these reserves are full, the remaining glucose is converted into body fat.
Fructose: This is found naturally in fruits but is also a significant component of corn syrup and table sugar. Fructose does not trigger an immediate spike in insulin because (unlike glucose) the majority of the cells in the body cannot use it. The liver can process fructose but, when large amounts of it are consumed (for example, in sugary soft drinks), the liver becomes overwhelmed and turns the fructose directly into fat. Ultimately, this contributes to non-alcoholic fatty liver disease (NAFLD).
Sucrose: This is a double molecule composed of 50% glucose and 50% fructose it is what is commonly called “table sugar.” Sucrose is particularly problematic as it both causes an insulin spike and also heads to the liver and is thus more damaging to metabolic health than either on their own.
Where does sugar come from in your diet?
Our sources of sugar are split into some primary types:
Simple carbohydrates (sugars): these (e.g. table sugar) are made of only a few component units, which enables the body to break them down very rapidly. These lead to a spike in insulin, and if the sugar is not quickly consumed, they are easily converted to fat. Simple carbohydrates thus provide an immediate source of energy.
Complex carbohydrates (starches): these (e.g. pasta, rice, potatoes and bread) are much longer chains of component units, and it takes the body significantly longer to break them down into individual glucose molecules. They provide a slower release form of energy.
Complex carbohydrates (fibre): these (e.g. leafy greens and whole grains) are carbohydrates that your body cannot break down. They pass through you without raising blood sugar or insulin levels – but do slow down and buffer the absorption of sugars consumed at the same time. Fibre is, however, an important source of food for your gut microbiome.
Why is sugar important?
Glucose is the primary source of fuel and is used in almost every cell in the body (e.g. our muscles and brain) to generate energy. There are two primary methods in which glucose is burnt, aerobic respiration (where you are not working hard enough to exhaust the available oxygen supply) and aerobic respiration (where your level of work is higher than the available oxygen supply). When you no longer have sufficient glucose available (for example, through restricting carbohydrate intake or through fasting), the body does have another available source of fuel. The liver can break down stored fat to produce small amounts of glucose (although nowhere near as much as that found in food) and ketones. You can think of ketones as the body’s ‘Plan B’ for when there isn’t enough sugar around. Specifically, ketones can cross from the blood to the brain and become the brain’s primary source of fuel when glucose levels are low.
What is insulin?
Insulin is the body’s primary storage hormone and has three specific roles:
Firstly, glucose cannot enter cells directly. Instead, insulin acts as a signal to the cells to open ‘doorways’ which allow the glucose to enter the cells to then be consumed to generate energy.
Secondly, when enough glucose is present, insulin instructs the muscles and liver to store the excess in the form of glycogen (which can be thought of as a short-term energy reservoir).
Finally, once the liver and muscle glycogen reservoirs are full, insulin instructs the body to store excess glucose as fat.
Critically, whilst insulin levels are high, the body will remain in storage mode and not release stored fat to use as fuel. The more sugar you consume and the more frequently you consume it, the higher your ongoing insulin levels are.
What happens when sugar intake is too high and/or too frequent?
The most well-known consequence of high insulin levels (due to diet) is that of type 2 diabetes. In this condition, the cells become resistant to the level of insulin in the blood, causing the body (specifically the pancreas) to manufacture more and more insulin to conquer the cells’ resistance. Eventually, this leads to burnout, with the pancreas unable to produce sufficient insulin and uncontrolled blood sugar levels. High blood sugar levels cause wide-ranging cellular damage across the body.
However, as noted at the start of this article (and the references at the end), there are a range of other consequences of high insulin levels.
A healthy, balanced diet which minimises simple carbohydrates and ultra-processed foods in conjunction with exercise, high quality sleep, and avoiding ‘snacking’ (to prevent continuously spiking insulin) is a way to avoid a lifestyle-induced drift into hyperinsulinemia, type 2 diabetes, and a range of other adverse health conditions.
Which monitor do I use?
I use the Abbott Lingo for which I pay £59 (convert this…).
The device is simple to apply, connects to my phone and lasts for 14 days. The app is straightforward to use and extremely useful for getting realtime feedback after meals and also for looking at what is happening whilst I am asleep. I also download all my data as a spreadsheet for my own analysis and for posterity.
What did I learn from monitoring my blood glucose?
It is worth noting that I am a vegetarian (for personal moral reasons rather than for health reasons). In fact, I follow a primarily plant-based diet apart from some occasional cheese or eggs (as part of family meals). I follow a time-restricted eating (TRE) lifestyle with a longer fast each week. I do not follow a ketogenic diet but avoid ultra-processed foods and simple carbohydrates. I was thus (arrogantly!) not expecting to get much out of using a continuous glucose monitor. However, the first time I used one, I gained some valuable insights:
-
I was able to identify a few often eaten foods I was consuming that were contributing to significant and totally unnecessary insulin spikes. Just a few examples were the use of oat milk in my lunchtime smoothie, homemade pop-corn as a healthy snack, and lentil cakes. Just a few simple adjustments removed those spikes and keep my glucose levels firmly in the normal range through day and night without changing much in my diet at all.
-
Even more valuably, I was able to see the impact of my late dinners (especially those after 8pm) on my nighttime metabolism and correlate nighttime sleep disruptions (as recorded on my Whoop) with elevated nighttime glucose levels (as recorded on my Lingo). As noted in the article on sleep, by shifting my eating hours to between 10 am and 4 pm, I was able to avoid the dreaded 3am wake-ups. Although I eat earlier I value family dinners, so I will still ’eat’ with my partner but just have a herbal tea. It’s a bit disruptive to family life, but the benefit in terms of sleep has been worth it!
-
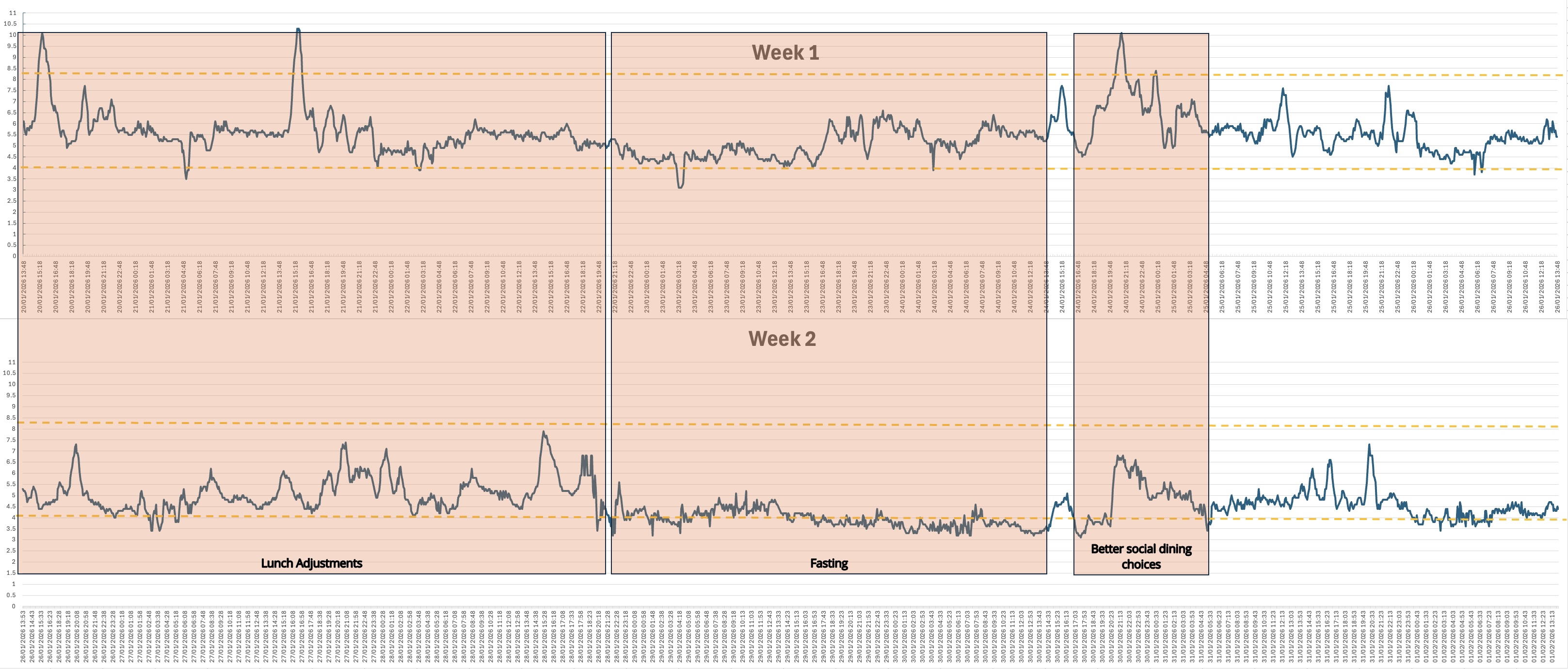
During my fast in week 2, my blood sugar was lower through the fast than in week 1, and my level of ketosis just before breaking the fast was higher in week 2 than week 1. This may suggest that better choices early in the week made it easier to get into ketosis later on in the week.
I downloaded all my data from the Lingo app, and the following graphs I generated may be interesting. The first covers Week 1 where I just ate as normal to gather baseline data and spot sugar spikes. The second covers Week 2 where I aimed to learn from Week 1 and keep my sugar levels within the normal range of 3.9-7.8 mmol/L (millimoles per litre). My average glucose across the whole of week 1 was 5.5 and across the whole of week 2 was 4.6 which was quite a considerable improvement.
Further sources of information
The Examine web site for independent, unsponsored meta-analyses of health research
Dr Robert Lustig on the Diary of a CEO podcast
Metabolical by Dr. Robert Lustig
Outlive: The Science and Art of Longevity by Pete Attia MD
The Obesity Code by Dr. Jason Fung
The Diabetes Code by Dr. Jason Fung
References
[1] Kahn, S. E., et al. (2021). “The relative contributions of insulin resistance and beta-cell dysfunction to the pathophysiology of Type 2 Diabetes.” The Lancet.
[2] F. W., & Griffin, J. L. (2023). “The role of insulin resistance and hyperinsulinemia in the pathogenesis of NAFLD.” Nature Reviews Endocrinology.
[3] Artunc, F., et al. (2024). “The kidney in metabolic syndrome: How insulin resistance drives chronic kidney disease.” Journal of the American Society of Nephrology.
[4] Pandolfi, A., et al. (2021). “The Role of Insulin Resistance in Endothelial Dysfunction and Thrombosis.” International Journal of Molecular Sciences.
[5] de la Monte, S. M. (2023). “The Evidence for Type 3 Diabetes and its Role in Alzheimer’s Disease Progression.” Journal of Alzheimer’s Disease.
[6] Gallagher, E. J., & LeRoith, D. (2020). “Insulin and Cancer: Integrative Physiology.” Endocrine Reviews.
[7] Swinburn, B. A., et al. (2019). “The Global Syndemic of Obesity, Undernutrition, and Climate Change: The Lancet Commission report.” The Lancet.
[8] Lustig, R. H., et al. (2022). “The Role of Processed Foods in the Pathogenesis of Metabolic Syndrome.” Frontiers in Nutrition.
[9] Hall, K. D., et al. (2019). “Ultra-Processed Diets Cause Excess Calorie Intake and Weight Gain: An Inpatient Randomized Controlled Trial of Ad Libitum Food Intake.” Cell Metabolism.