

Monitor Your Heart Health
Check and track your blood pressure regularly. Use blood testing to monitor levels of key markers and uses scans to check for the presence of plaque buildup in your arteries.
Why should you care about heart health?
Cardiovascular disease (CVD) is the leading cause of death globally [1] so anything you can learn about your genetic propensity to suffer from it, your current cardiovascular health, and the impact of your diet and lifestyle can help you to mitigate the risk. It’s important to note that the vascular damage that ultimately leads to incidents like a heart attack or a stroke starts long before the actual event and, despite there being a genetic aspect to this condition, there is much that can be done in terms of diet, lifestyle and exercise. In fact, should you find out that you do have a higher genetic risk, then knowing that makes it even more important to take early action and make long-term changes.
Want to look at the science later but, right now, you are just interested in some actions to take?
Let’s start with a couple of key definitions and by clearing up one common confusion.
First, what exactly do we mean by the term Cardiovascular Disease (CVD)? CVD is an umbrella term that encompasses a systematic decline affecting the heart and blood vessels (arteries, veins and capillaries). We can unpack it a bit further into the following specific conditions:
- Coronary Artery Disease (CAD): The hardening and narrowing (due to the build-up of plaque) of the arteries supplying the heart. This can lead to chest pain (angina) or myocardial infarction (MI) (a heart attack) whereby plaque ruptures and a fragment fully or partially blocks an artery supplying the heart.
- Cerebrovascular Disease (Stroke): This is similar to coronary artery disease, but instead affects the blood vessels supplying the brain. The incident could be caused by a blockage (an ischaemic stroke) or by a bleed (often due to high blood pressure leading to a burst vessel).
- Peripheral Arterial Disease (PAD): In this case the damage is to the arteries in the legs and arms leading to pain and even tissue death.
- Aortic Aneurysm and Dissection: Here the impact is felt in the aorta (the largest artery in the body) and manifests as weakness/bulging (aneurysm) or a rupture (dissection). There is a strong link between this condition and unmanaged high blood pressure.
Before we get to the checks you can make and the tests you can have performed to keep a close watch on your heart health, let’s clear up some confusion and old-fashioned language around cholesterol and the risk of CVD. The following statement is something you might well be familiar with but is both inaccurate and untrue:
Let’s pick this statement apart and correct it before we go any further! Firstly, cholesterol is not ‘bad for you’, it’s actually a fundamental building block of human life with a number of key roles such as:
- Contributing to the formation and stability of cell walls
- Helping to create hormones such as testosterone, estrogen, and cortisol
- Helping in the synthesis of vitamin D and in the production of bile salts in the liver.
Without a healthy level of cholesterol, quite simply, you would die and in fact, the majority of cholesterol is manufactured by your body, with only a minor portion coming from your diet. Thus, dietary approaches focused on reducing cholesterol are quite clearly nonsense. The issue does not lie with cholesterol itself. It lies with how cholesterol is transported around the body. Because cholesterol belongs to the lipids family (fats) it is not soluble and yet must be transported in the bloodstream. The way the human body achieves this is to wrap cholesterol up in spherical particles called lipoproteins, which are water-soluble. You can think of the lipoproteins as little boats which carry the cholesterol around the body. Lipoproteins are protein on the outside and lipid on the inside - hence their ability to both hold cholestrol and be transported in the blood. It is not the cholesterol that is bad - it’s the nature of some of the particles carrying it. There are two classes of lipoprotein you need to care about (and we’ll look more at this in the section on testing below).
- Low Density Lipoproteins (LDL): These carry more lipid in relation to protein and thus are less dense. Speaking simplistically, these are the ‘bad ones’
- High Density Lipoproteins (HDL): These carry more protein in relation to lipid and thus are denser. Again, simplistically, these are the ‘good ones’
Let’s get a bit more specific so that you are ready for when we look at blood tests shortly. LDL (the bad, low-density ones) are wrapped in a molecule called apolipoprotein B (apoB) whereas HDL (the good, high-density ones) are wrapped in a molecule called apolipoprotein A (apoA). Every lipoprotein (not just LDL but also others) that contributes to arterial damage carries apoB.
So, if it’s not cholesterol ‘blocking up’ your arteries, then what exactly is the damage that LDL (with its apoB marker) is causing? The key term here is atherosclerosis, which is the thickening and hardening of the inner wall of the arteries due to the build of plaque. In essence, the LDL (apoB) tends to stick to the inner wall of the artery (called the endothelium) and has an inflammatory and damaging effect leading to lesions on the artery wall. When there is significant LDL (apoB) present, it is the body’s efforts to tackle this damage that ultimately leads to fatty streaks (the precursor of plaque) forming on the artery walls. Specifically, as the body dispatches soldiers (called macrophages) to swallow up oxidised (effectively rancid) LDL stuck to the lining of the arteries those macrophages themselves can ingest too much of the cholesterol carried within the LDL and blow up to form a kind of foam. Given enough of this foam, a fatty streak forms, which is the core of the arterial plaque that forms as the body tries to build a barrier. This soft plaque is harder to detect (see scans later) but, over time, it will become hardened with calcium deposits. At this point the atherosclerosis is quite advanced and is more easily detectable. HDL (aopA) is considered to be good because it has the opposite effect and can pull the cholesterol back out of these macrophages and ship it back into the blood stream.
Thus, a much better version of that erroneous earlier statement would be:
I’m unapologetic if this seems like a much more complex statement. If you want to take some ownership of your heart health, then the results of your blood tests are critical information that you need to know how to interpret properly.
Before we move on, let’s conclude with a look at some specific lipoproteins of particular concern and also discuss the role of triglycerides (as you are going to see those pop up on your blood tests also).
- Very Low Density Lipoprotein (VLDL): These lipoproteins are carrying mostly Triglycerides (fuel created by consuming more calories than are required) and a little bit of cholesterol. They are very light (due to the higher relative levels of fat) and large and are thus very low density when compared to LDL. They are concerning because once they have dropped off their triglyceride payload, the remnant is highly inflammatory and triggers an immune response in the arteries.
- Triglycerides: Are a type of lipid (fat) that are created when your body consumes more calories than are needed (effectively creating a reserve of spare energy). Triglycerides are increased by eating fatty ultra processed foods (e.g. trans-fats) and by consuming sugary drinks and foods. There are a number of reasons to care about triglycerides (e.g. they lower your good HDL and make your blood more ‘sticky’ and likely to clot), but the primary concern is that their presence leads directly to the formation of the previously mentioned VLDL (very low-density lipoprotein).
- Small, Dense Lipoproteins: After the VLDL has dropped off its cargo of Triglycerides, it shrinks and becomes denser since it is now predominantly protein and cholesterol rather than fat (becoming the LDL we are familiar with already). However, when the levels of Triglycerides are high, after the LDL has dumped its cargo of Triglycerides, it will then be forced to drop its remaining cholesterol and take up even more Triglycerides. When these particles pass through the liver, an enzyme called hepatic lipase rips the Triglycerides out of them, causing them to collapse into small, dense particles with a higher percentage of the bad apoB protein compared to the fat inside. These small dense lipoproteins are dangerous as they are both inflammatory and their smaller size enables them to more easily penetrate the lining of the arteries.
- Lipoprotein(a) - abbreviated to Lp(a): Is formed when normal LDL fuses with a “kinked” protein string called Apolipoprotein(a) (don’t confuse this with the very similarly named apoA that we discussed earlier as a marker for good HDL!). The resulting structure is very effective at collecting up unpleasant oxidised lipids as it passes through the blood and then penetrating the lining of the arteries with this payload. The level of Lp(a) is controlled almost entirely by genetics and is not currently amenable to any medication or dietary influence. Around 20-30% of the population has levels high enough to create a risk, and a specific blood test can allow you to check yours (see below). It’s a ‘once a lifetime’ test as there is nothing you can currently do about it, however, knowing you have this vulnerability enables you to double down on every other aspect of cardiac health to ensure all the risks you can control are as tightly managed as possible. In addition, gene silencing techniques are probably only a few years away, so, if you have this genetic pre-disposition, it’s important to do everything else you can to buy time until new therapies are available. Lp(a) is also hazardous as it is NOT routinely included in a lipid panel, and it is possible for other markers to look good whilst this, untested one, runs rampant. It is even more important to get tested for Lp(a) if you have any familial history of heart attack.
Armed with all this information, you now have a decent chance of interpreting the information you can gather. So, let’s get back to what you can practically do to keep a close eye on your cardiovascular health:
- Regular blood testing to look at key markers (such as apoA and apoB).
- Once in your life testing to look for a genetic susceptibility to Lp(a).
- Daily checking and tracking of your own blood pressure at home.
- Scanning such as a Coronary Calcium (CT) scan or a CT Coronary Angiogram (CTCA) to actively visualise your arteries.
Testing of blood (a lipids panel)
You may well find (given your age, ethnicity, and family history) that your health care provider is running regular blood tests, but, if not, you can easily commission these yourself using an at-home blood draw service. I use Thriva but many other providers exist. What is essential is that your provider includes tests for apoA and apoB and also offers an optional extra test for Lp(a). You are (as we saw earlier) not interested in vague assertions and statements about cholesterol – you need the real data! Your testing provider (or, of course, your doctor) should also provide a report to help you interpret the results.
Here’s what you can expect to see in your lipids panel results:
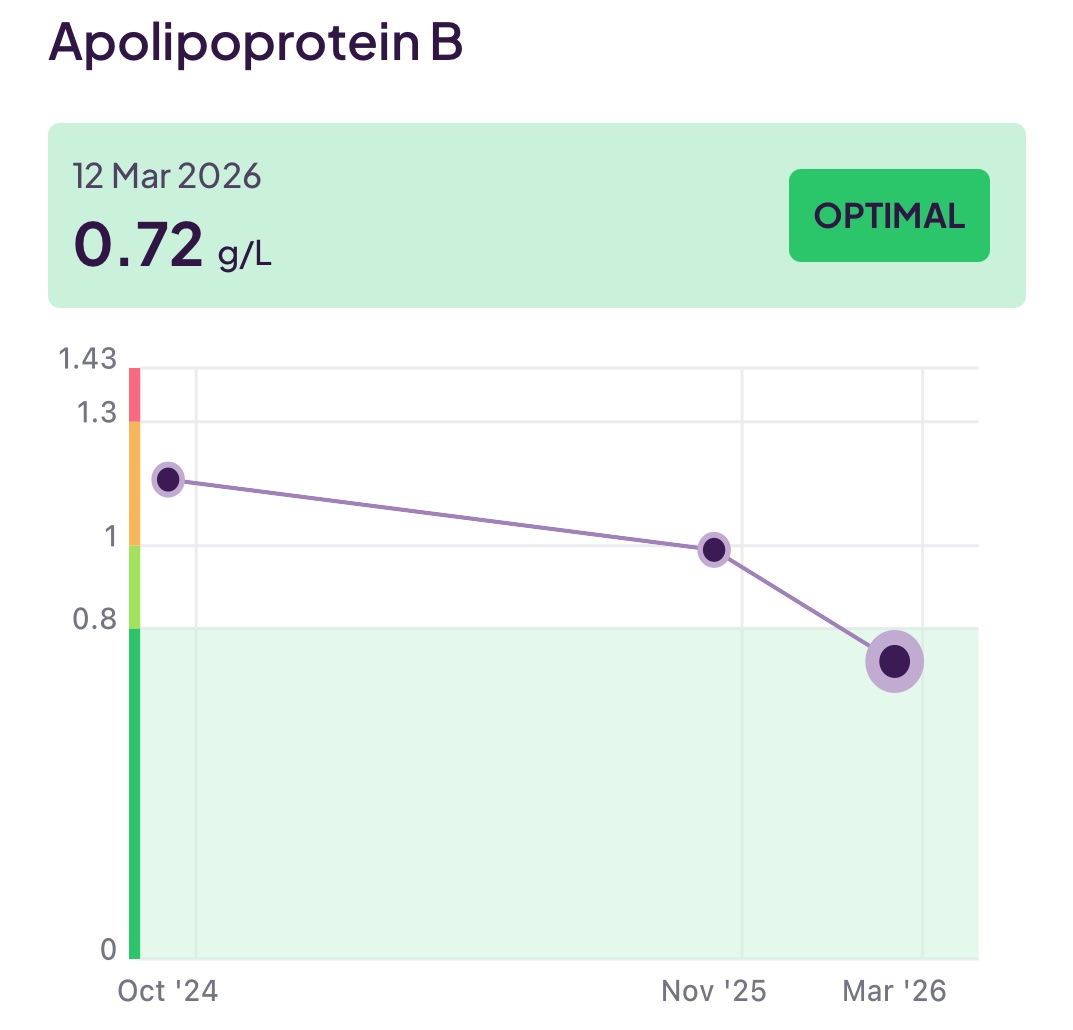
- Apolipoprotein B (apoB): This is the marker for bad lipoproteins that damage your arteries, and you want this to be low and to trend lower over time if it is initially high.
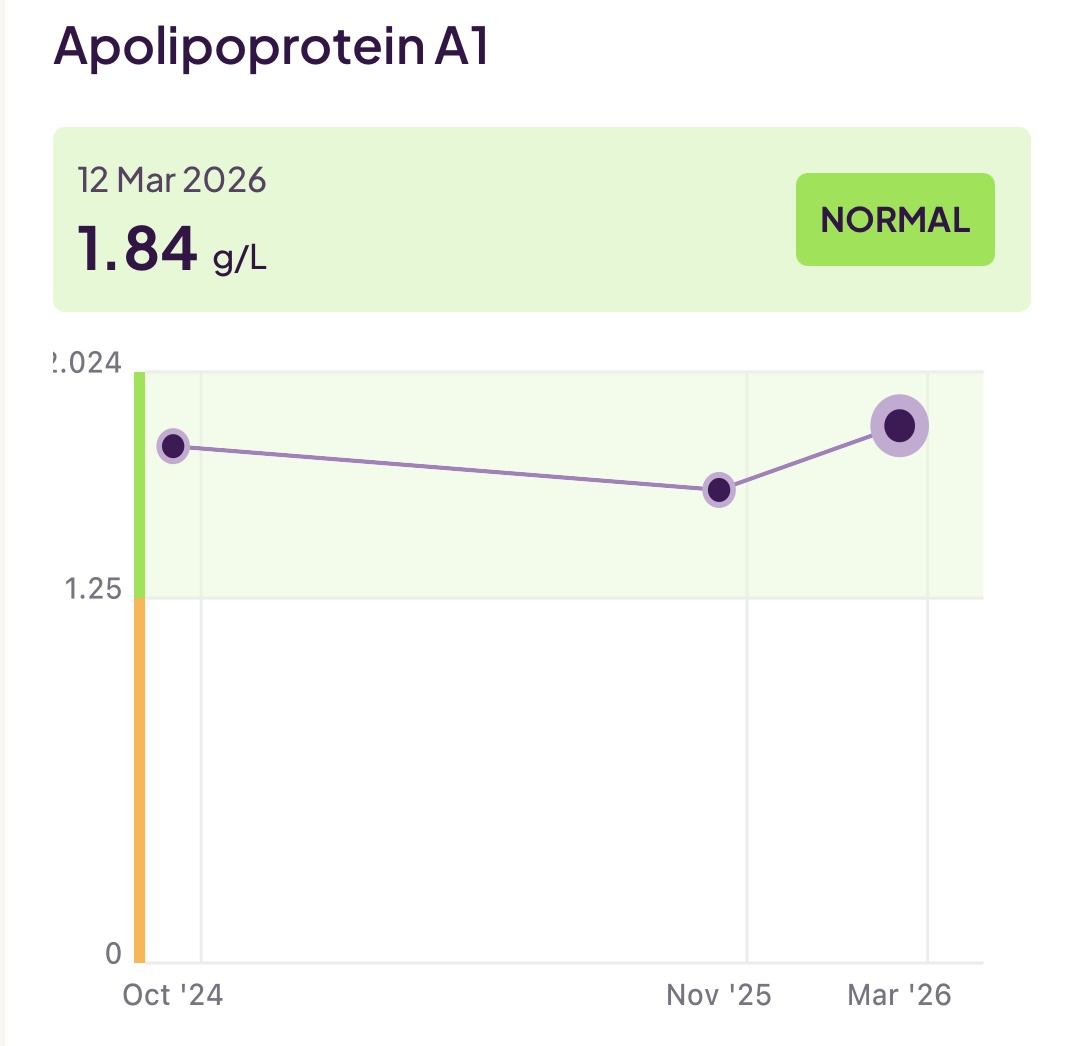
- Apolipoprotein A (apoA): As we saw earlier, this is a key marker for good lipoprotein that protects your heart health. You want this (unlike most lipid test results!) to be as high as possible, and you want to actively work to get it up over time if it is initially low.
- ApoB:ApoA ratio: You want your good (apoA) to dominate your bad (apoB) so you want a lower number for this ratio and to see it trend down.
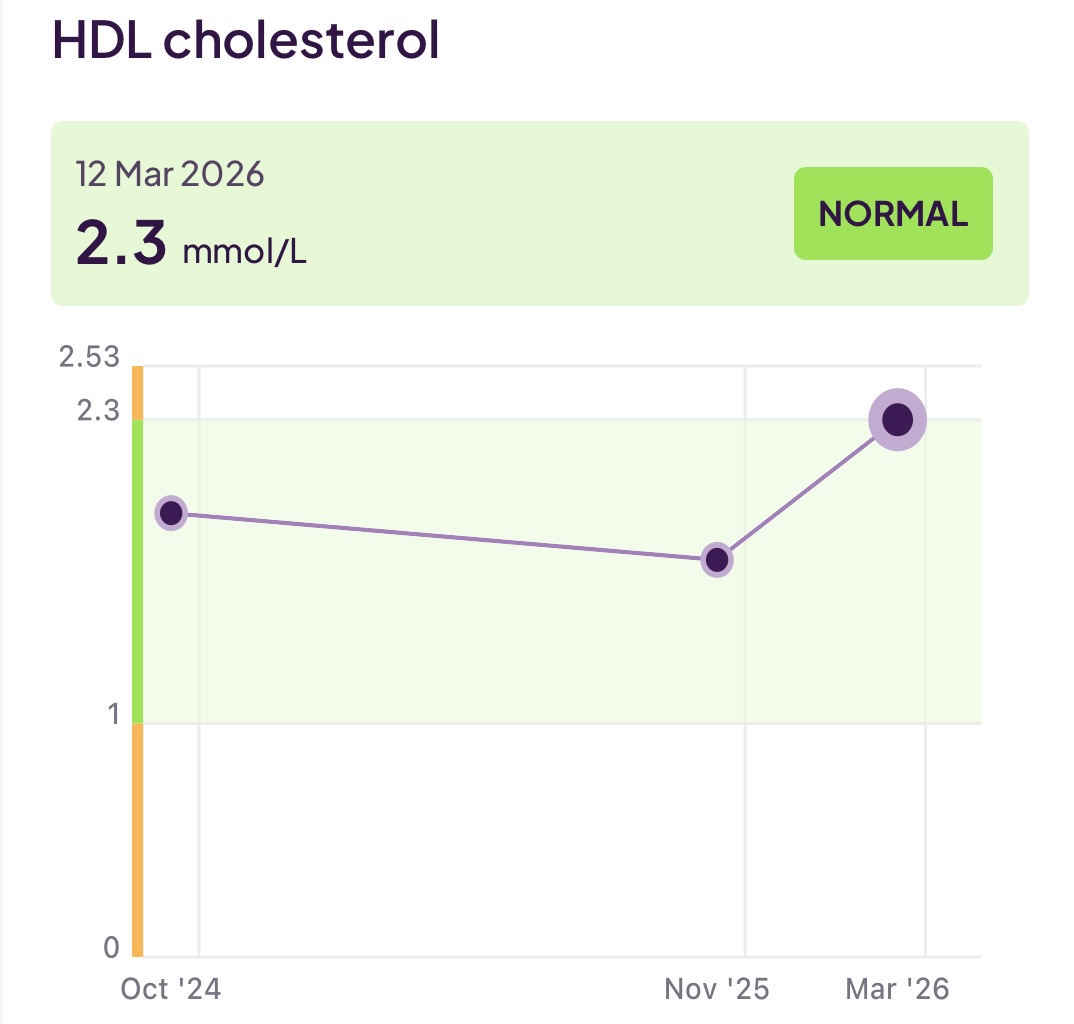
- High Density Lipoproteins (HDL): You may be more familiar with this measure from older tests. Nowadays (as discussed) apoA is a better predictor, but your panel will still include this value, and you would expect it to trend with your apoA reading
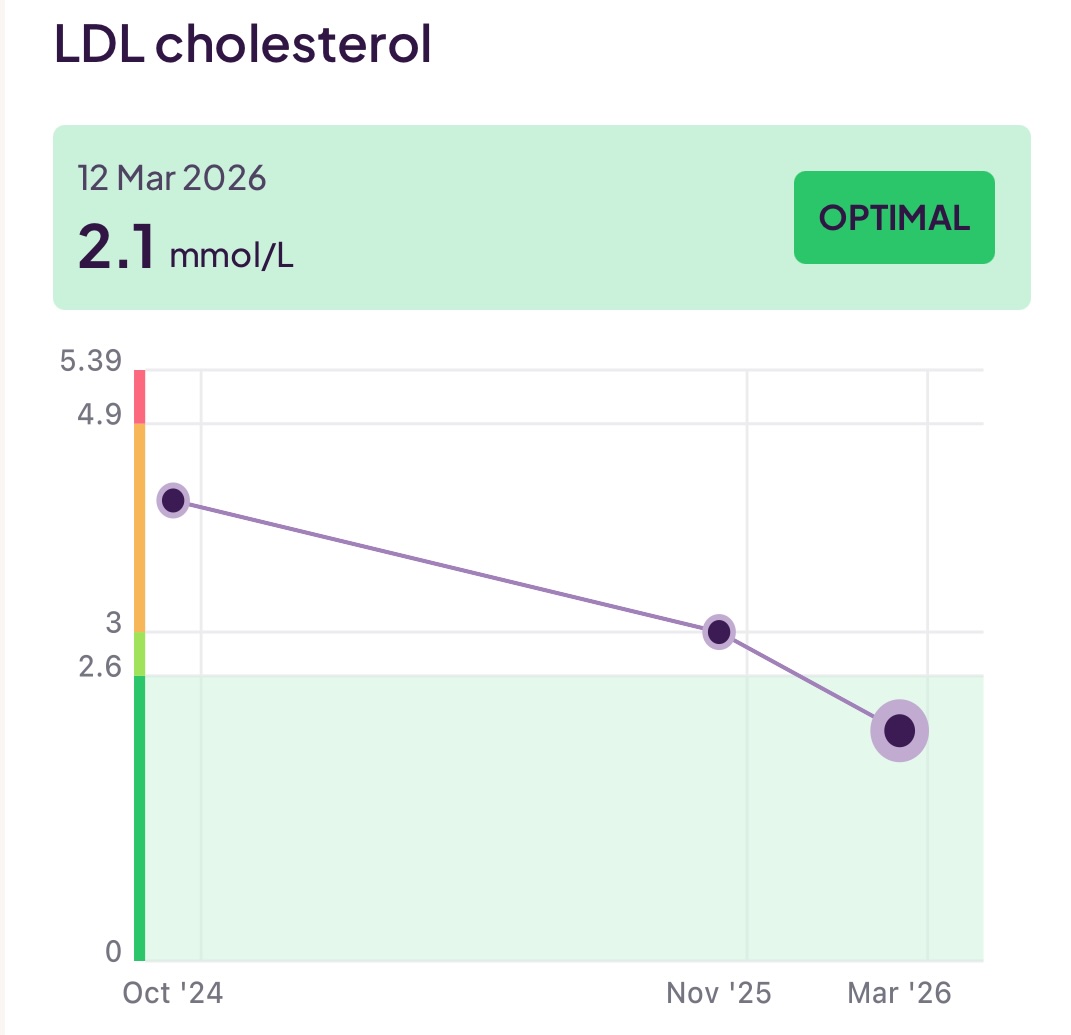
- Low Density Lipoproteins (LDL): Again, apoB is now a better predictor than the amount of cholesterol carried by LDL particles, but the value will still be in your panel and follow your apoB level
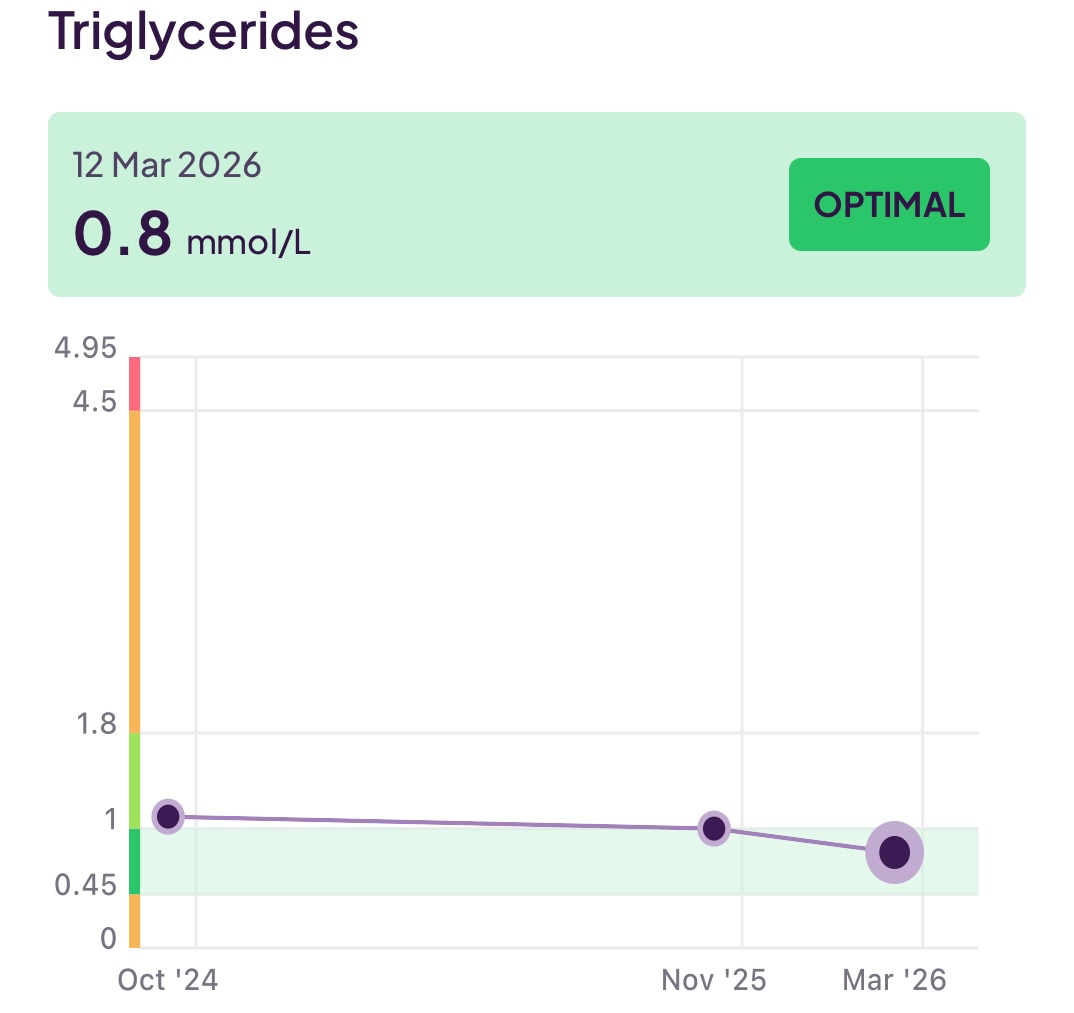
- Triglycerides: This is the measure of triglycerides in your blood which, as mentioned earlier, contribute to the presence of dangerous Very Low Density Lipoproteins (VLDL) and, subsequently, the also dangerous small dense lipoproteins. If your Triglycerides are elevated, you want, as a priority, to make diet and lifestyle changes to address this.
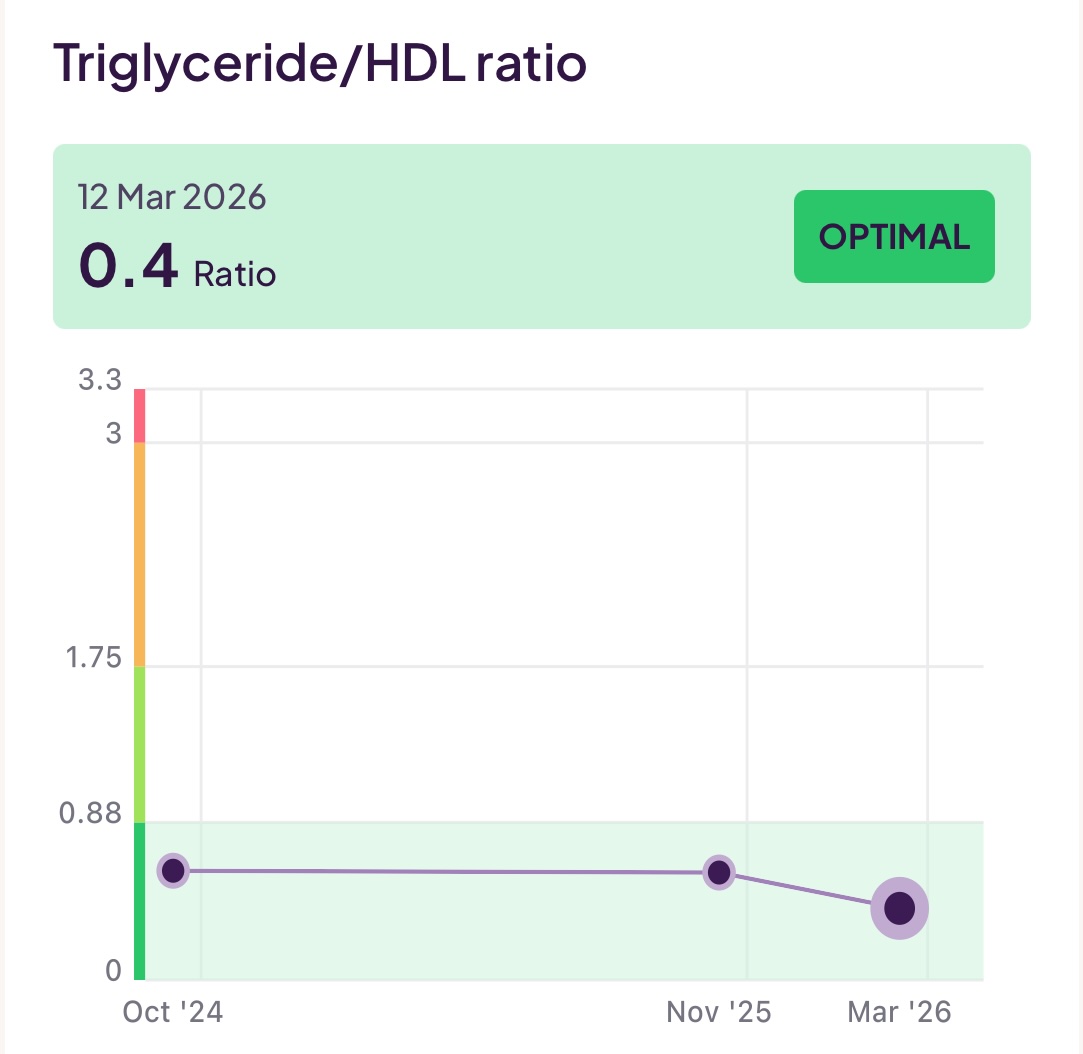
- Triglycerides/HDL Ratio: This is another useful measure because it gives you a clue as to the levels of the dangerous small, dense lipoproteins we discussed earlier. Even if you have LDL levels within a normal range, if this ratio is high, you may still be at risk from small dense lipoproteins.
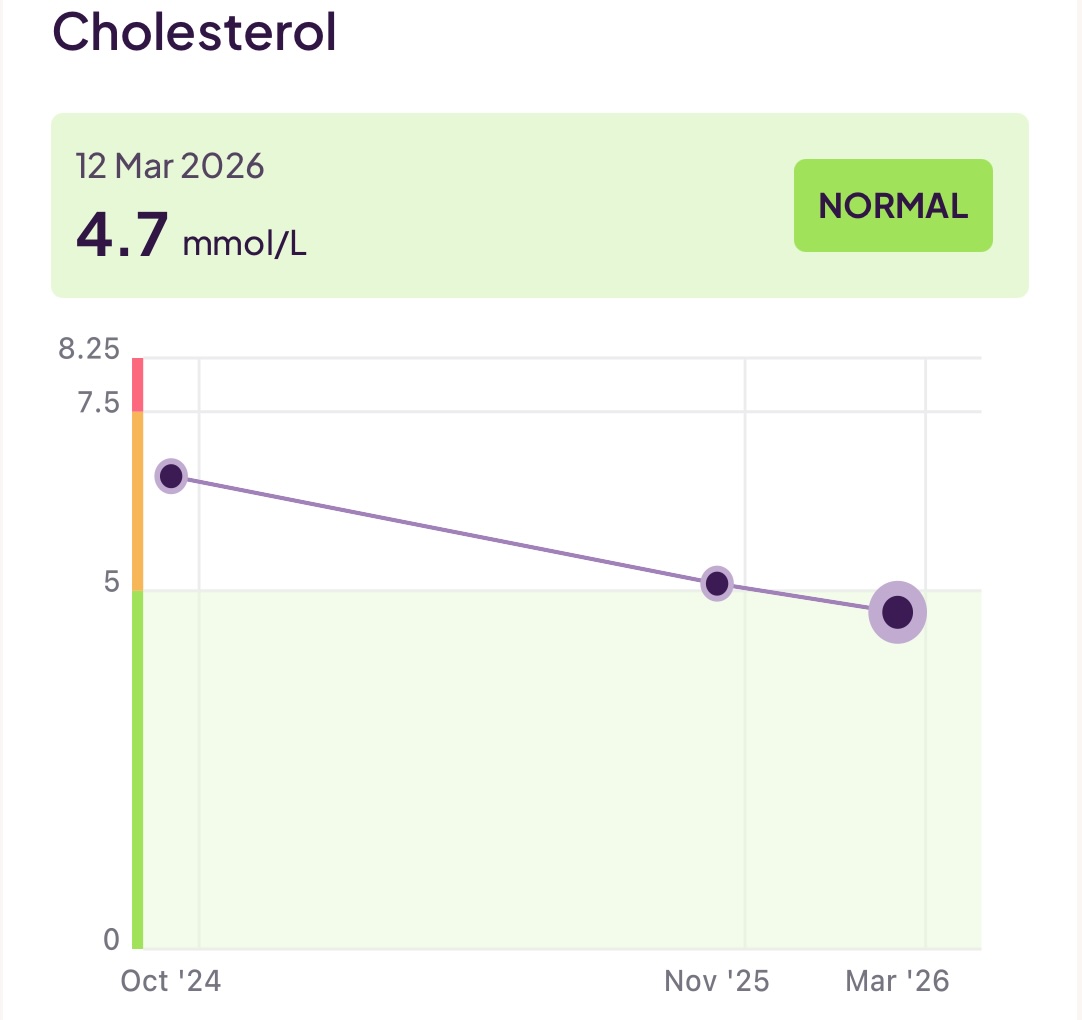
- Cholesterol: This is the measure of cholesterol in your blood. As we have already discussed, we are much more interested in what is carrying cholesterol than in the cholesterol itself. This is just the sum of both the cholesterol carried by (good) apoA lipoproteins and (bad) apoB lipoproteins. It tells us nothing about the ratio of those.
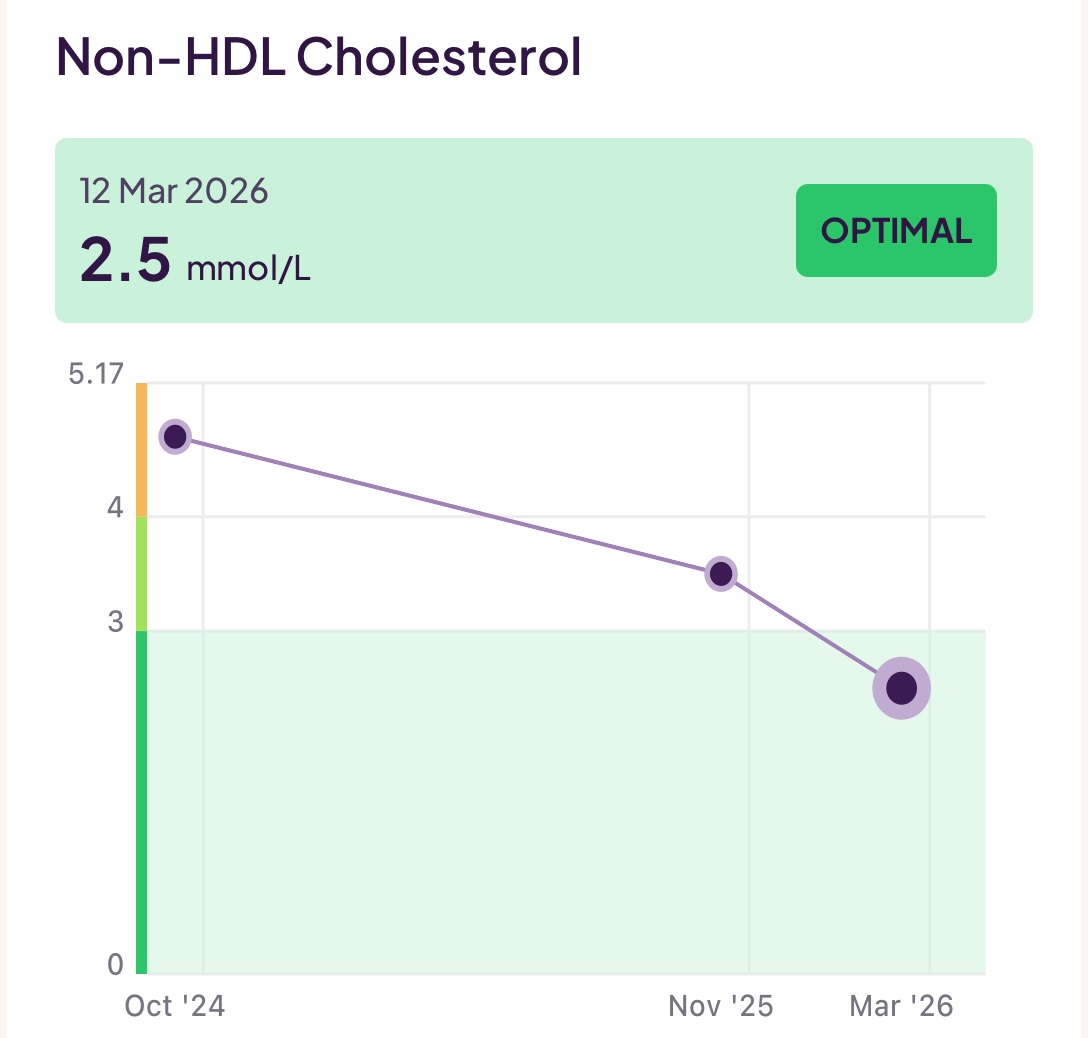
- Non-HDL Cholesterol: This is your total cholesterol minus the cholesterol carried by the good HDL lipoproteins. This is interesting because the value is the sum of your (bad) LDL and also other lipids such as the dangerous very low-density lipoproteins (VLDL). If you thus subtract your LDL value from this value, you can get a feel for your levels of VLDL.
I have been working to reduce the amount of (bad) LDL (aopB) whilst increasing the levels of good HDL (apoA) and also keeping an eye on my triglycerides. To make all the above discussions more real, you can see 18 months of my test results below:

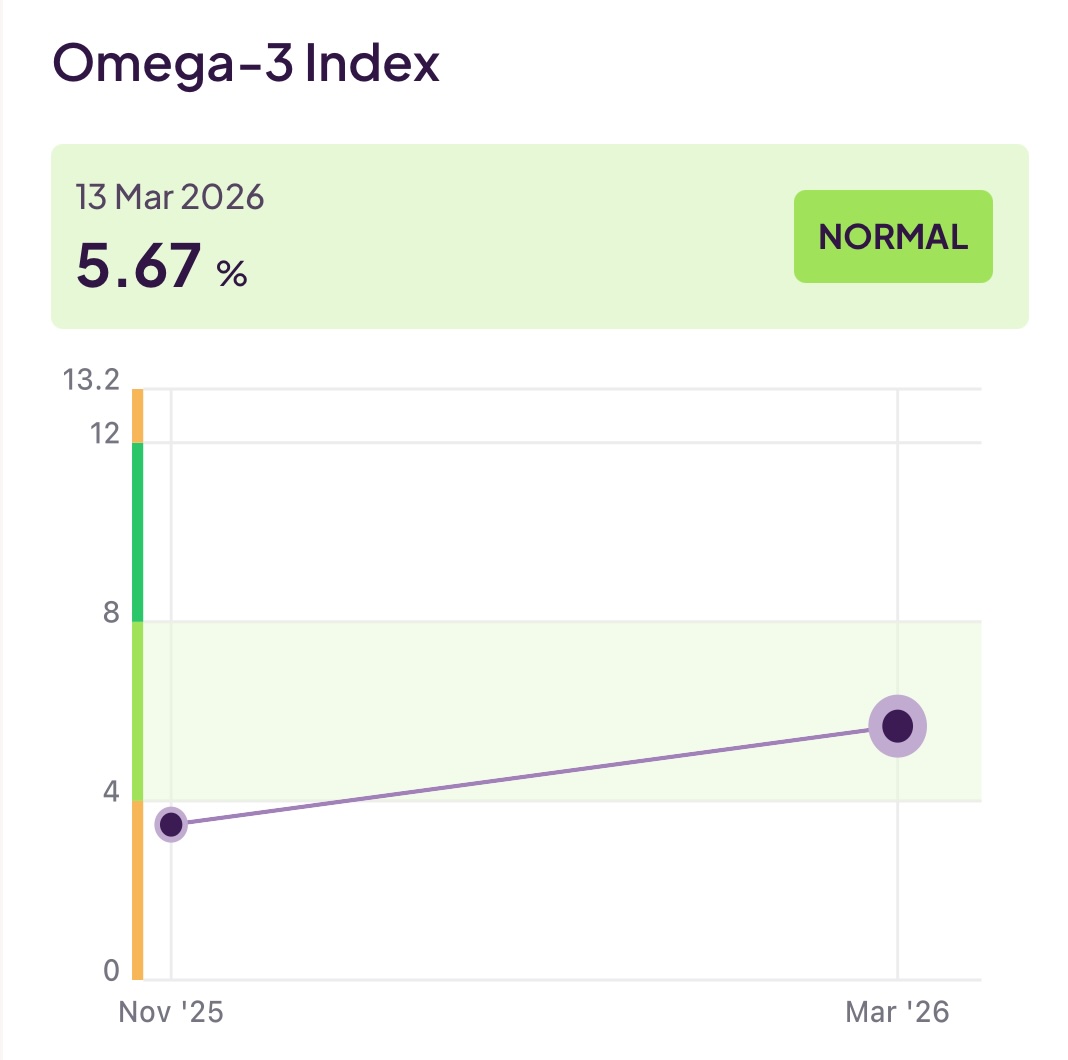
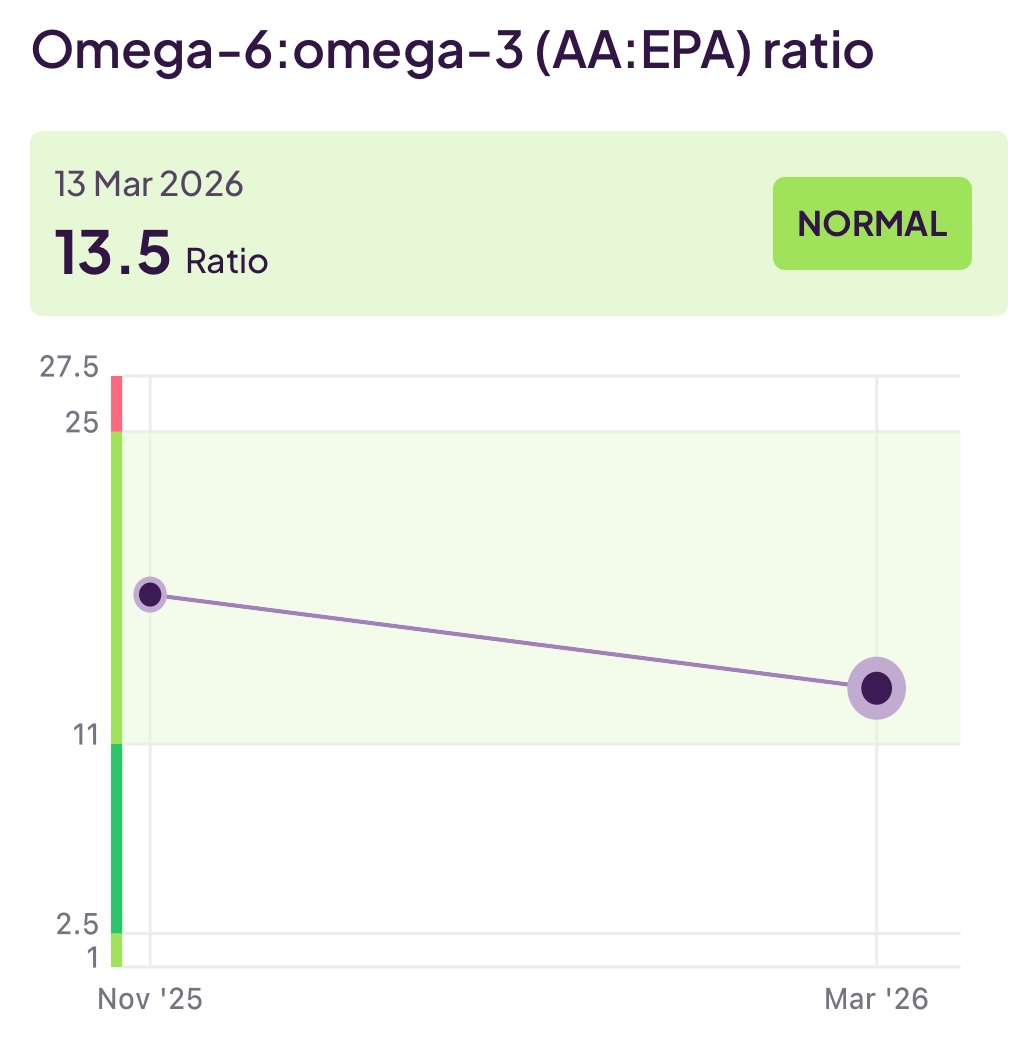
Although not (always) included in a lipid panel, another useful set of tests would be your Omega-3 level, Omega-6 level, and the ratio between them. Omega-3 and Omega-6 are unsaturated fats and both are essential for health. Specifically, Omega-3 has an anti-inflammatory effect, whereas Omega-6 has an inflammatory effect. If (as is the case for many people on a modern diet) the amount of Omega-6 dominates over Omega-3, you can increase your cardiovascular risk.
You can read lots more about Omega-3 and Omega-6 in Big10 #5 (Design Your Personal Supplement Stack Informed by Blood Testing)
Below you can see my recent Omega-3 and Omega-6 levels. As someone with a predominantly plant-based diet, this testing exposed to me that the supplement I was taking for Omega-3 just wasn’t cutting it and prompted me to switch to a more potent form. This has helped a bit, but there is still more to do. Most likely I will increase further the amount of my Omega-3 supplement. My diet is very healthy and avoids processed foods and seed oils, so I strongly suspect that the high Omega-6 levels are coming from things I don’t want to cut out (like nuts, seeds, tofu). Thus, an approach based on further increasing Omega-3 is my plan for now.
Genetic susceptibility testing
Earlier on we looked at Lipoprotein(a) – abbreviated to Lp(a) – and discussed that this was a particularly inflammatory lipoprotein whose risk is predominantly driven by genetics and is not amenable (currently) to management by either lifestyle or medications. Routine lipid panels (blood tests for heart health) don’t include it, but you should request or order this ‘once in a lifetime’ test.
If you do find out that you have elevated levels of Lp(a), you should take even more seriously the heart health measures we will look at later on in this article. The fact that you cannot change your Lp(a) levels should not be a reason to give up, in fact quite the reverse, it should be a motivation to stack all the other odds in your favour!
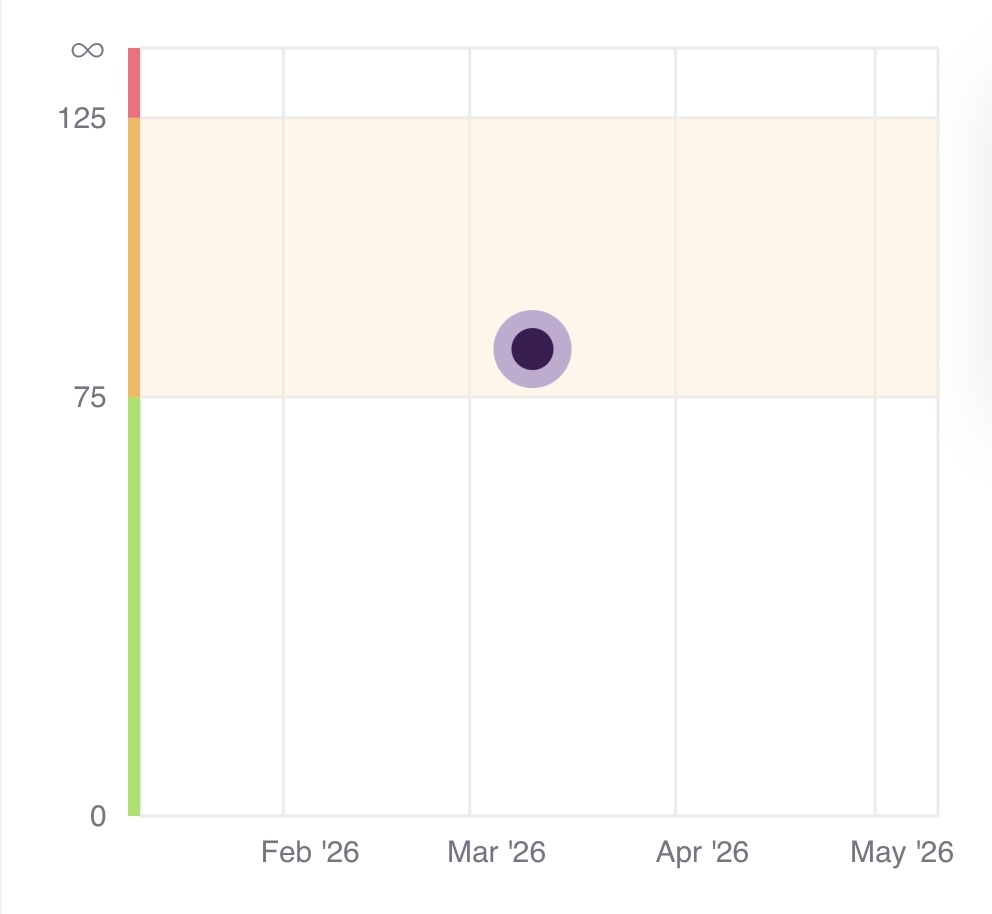
Sadly, for me, I did test positive for this with levels at the top of the minor risk range. The ranges are defined as follows:
- 32-90 nmol/L (minor risk)
- 90-200 nmol/L (moderate risk)
- 200-400 nmol/L (high risk)
- More than 400nmol/L (very high risk)
With my result being: 86 nmol/l
So, what can you do if you too find out you have elevated Lp(a) levels?
The good news is that there is a new class of drugs, currently in clinical trials, which have shown the ability to reduce Lp(a) levels by 80% to 95%. These are NOT currently approved but show great promise and may be as little as 2-3 years out. So rather than despairing, I would urge you to think about taking every possible measure (see diet and lifestyle changes below) to buy yourself the time to allow such treatments to hit the market. If you would like to find out more about these drugs and track their progress, have a look at:
- Technique: Small Interfering RNA (siRNA)
- Technique: Antisense Oligonucleotides (ASO)
- Drug: Olpasiran (uses siRNA)
- Drug: Pelacarsen (use ASO)
For people with high risk Lp(a) levels, there are also two techniques which aim to reduce the level of Lp(a) (as opposed to the emerging treatments mentioned before, which aim to turn Lp(a) off at the source):
- PCSK9 Inhibitors: These are primarily for lowering LDL, but can also reduce Lp(a) levels.
- Apheresis: This is a physical process where your blood is filtered through a machine to remove Lp(a). It is highly effective but usually reserved for people with extreme genetic cases and existing heart disease because it is expensive and time-consuming.
Noting all of the above, the other obvious management plan for Lp(a) is to stick fast to the diet and lifestyle advocated throughout the Big10. Specifically though:
- Drive apoB as low as possible: If your Lp(a) is high, your target for LDL/ApoB should be much lower than the “normal” range.
- Aim for optimal blood pressure to avoid the impact of mechanical stress on your arteries.
For me, although my apoB was 0.72 g/L at the last time of testing, this is only just inside the optimal/ low-risk range, so I continue my work to drive this down through a diet high in fibre and low in saturated fats and sugars coupled with exercise. I would like to see if I can aggressively drive apoB down to at least 0.5 g/l or even further so I am also discussing with my doctor going onto statins as that will provide an additional lever. In addition, as seen earlier, I am also focused on correcting my Omega-6:Omega-3 ratio.
In the section ‘Diet and Lifestyle’ below you can find lots more information on changes you can make to improve heart health
Blood pressure monitoring
Your blood pressure is one of the simplest (and most important) pieces of data you can gather on your own health, and yet it is remarkable how few people routinely (or ever!) check it. Elevated blood pressure is a significant red flag for cardiovascular ill-health and is closely related to your risk of cardiovascular disease, heart attack, and stroke. In the section we look at:
- The mechanics of blood pressure (i.e. what causes it to be elevated) and the impact of high (and low) blood pressure
- The ’notation’ used for blood pressure readings
- How you can check and monitor your blood pressure on an ongoing basis
The mechanics of blood pressure
As your heart beats to pump blood around your body, this will naturally generate pressure against the inside of your arteries. Further down you can see how this pressure is measured, but, for the moment, let’s just consider the mechanical factors in play that could cause that pressure to be higher than desired.
At a (very!) basic level your heart is simply a pump pushing fluid through a network of pipes (i.e a closed loop hydraulic system). Thus, thinking about the dynamics of fluids, the factors affecting pressure in such a system would be:
- The flow rate: In essence, this is how much fluid (blood) the pump (your heart) is moving every second. Flow rate is driven by the amount of fluid the pump ejects into the pipes and how often the pump strokes (beats) The pressure in your arteries will thus increase if your heart forces more blood through them per second.
- The resistance: This is how difficult it is to push the fluid through the pipe network (blood through your arteries). Resistance is increased by how viscous (sticky) the fluid is, the length of the pipe network (arteries) and (most critically) the radius of the pipes (arteries). Radius has a huge impact on resistance (e.g. just at 10% decrease in radius leads to almost a doubling of resistance).
The overall pressure in the system (your blood pressure) is calculated by multiplying the flow rate by the resistance. It is worth noting that a key difference from our pump/pipes example is that your arteries are flexible and thus much more capable of handling sudden spikes in pressure (think flexible rubber hoses vs rigid copper pipes).
Your blood pressure is thus clearly going to vary in a completely healthy way (e.g. due to exercise) but also in unhealthy ways (e.g due to poor cardiovascular health). Transient changes in your blood pressure (e.g. due to exercise load, standing up, increased ambient temperature, sleeping, digesting etc) are perfectly normal and a sign of a healthy and responsive cardiovascular system. However, what you need to be concerned about is when your blood pressure is ‘stuck’ at a high level – indicating an underlying issue such as increased resistance in your arteries due to blockages.
Do also be aware that persistently low blood pressure (or sudden sharp drops in blood pressure) is also a cause for concern and should also be discussed with your doctor. This is also true for irregularities in the beating of your heart (arrhythmia) - which some blood pressure monitors can also identify.
So, if your blood pressure readings are consistently elevated (see further down for the normal blood pressure range), what might be some of the possible factors involved?
- Arterial stiffening (e.g. a breakdown of elastin in the artery walls or a decreased ability of the arteries to expand and contract as required)
- Arterial narrowing (e.g. the buildup of plaque reducing the cross-section of the artery)
- Increased blood volume (e.g. high salt levels will require more water in the system thus increasing the volume of blood your heart needs to push around)
- Chronic stress (e.g. high cortisol levels causing an ongoing increase in heart rate due to a ‘fight or flight’ reaction)
Understanding a blood pressure reading
When a monitor is used to measure your blood pressure (something you can easily do at home), it records the result as two numbers with a slash between them. For example 118/70. The first number is your blood pressure (in mm of mercury – mmHg) when your heart pumps blood out and is called the systolic blood pressure. The second number is your blood pressure between beats and is called the diastolic blood pressure. Specifically:
- Systolic pressure: This is the maximum pressure against your artery walls as the heart’s left ventricle contracts to push blood around your body.
- Diastolic pressure: This is the pressure exerted as (between beats) your arteries recoil (since they are elastic) and keep the blood moving forward even whilst the heart is resting.
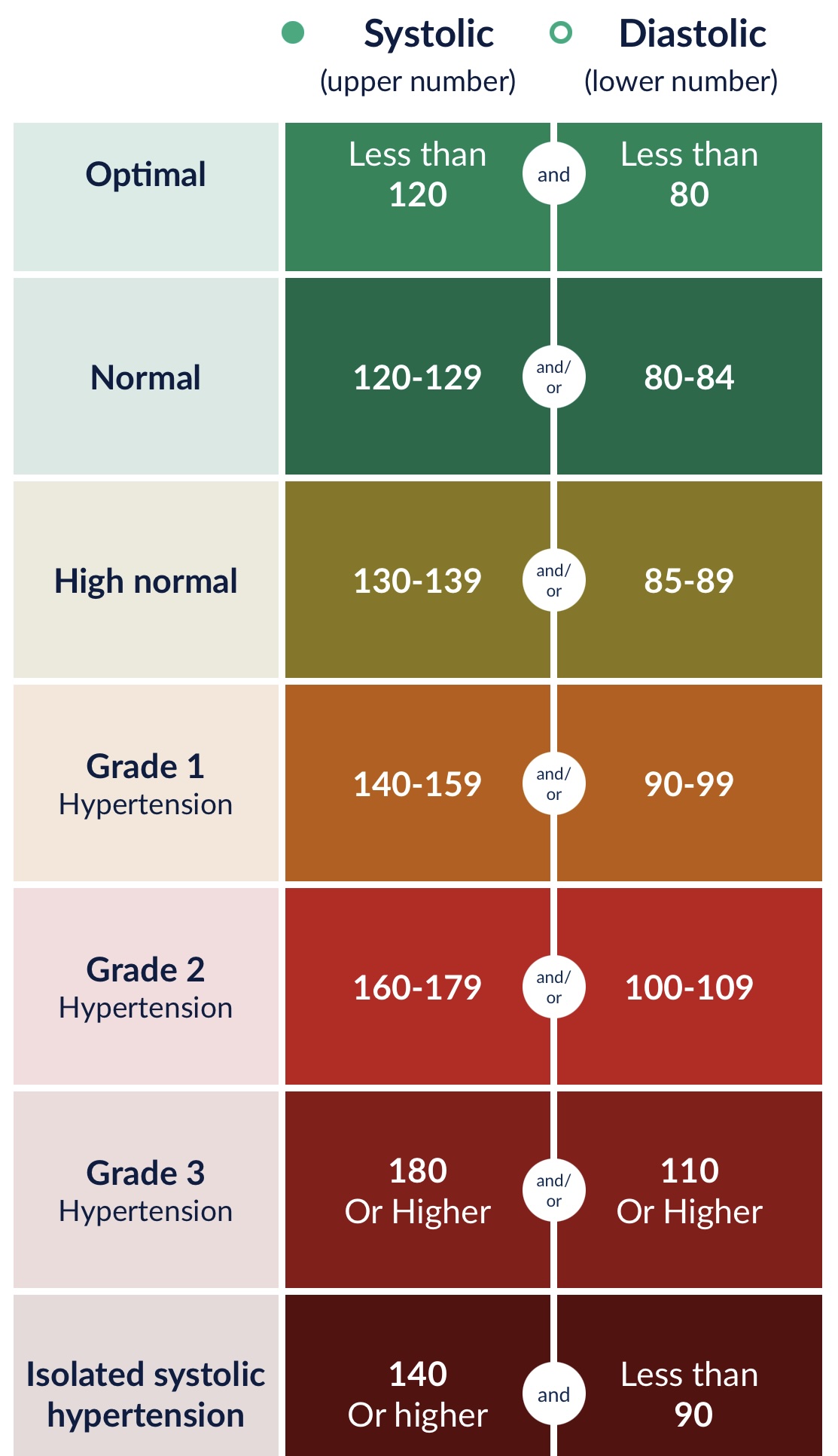
The ‘official’ values for what constitutes normal vs elevated blood pressure have changed over the years, but the current ESH (European Society of Hypertension) guidelines are as follows:
Taking and tracking your blood pressure
You can purchase a blood pressure monitor yourself and then check your own blood pressure regularly. I use (and find very convenient) the OMRON EVOLV Wireless Monitor which sends the readings straight to their app on your phone, which then synchronises them with Apple Health. There are, however, some specific things to keep in mind when purchasing a blood pressure monitor to ensure that you get one which is providing accurate values (and continues to do so over time):
- Upper arm only – don’t waste your time or money or wrist or finger monitors.
- Ensure it has been clinically validated as you want absolute confidence in the values it gives you. In the UK look for British and Irish Hypertension Society (BIHS) seal of approval. In the US: Look for the AMA (American Medical Association) “Validated Device Listing” (VDL) or the AAMI (Association for the Advancement of Medical Instrumentation) standard.
- Ensure it clearly states how long the device is guaranteed to remain accurate for before it must be returned for servicing (or replaced)
- Check the minimum and maximum cuff size against your arm mid-upper arm diameter as this is a very common cause of inaccurate readings.
- Look for reputable suppliers and don’t base your decision on price
- You’ll be doing this daily, so a little extra investment for one that is convenient to use and well integrated is worth it
Don’t forget to take your blood pressure at the same time(s) each day and do it whilst at rest and comfortable so that you are getting comparable, consistent readings.
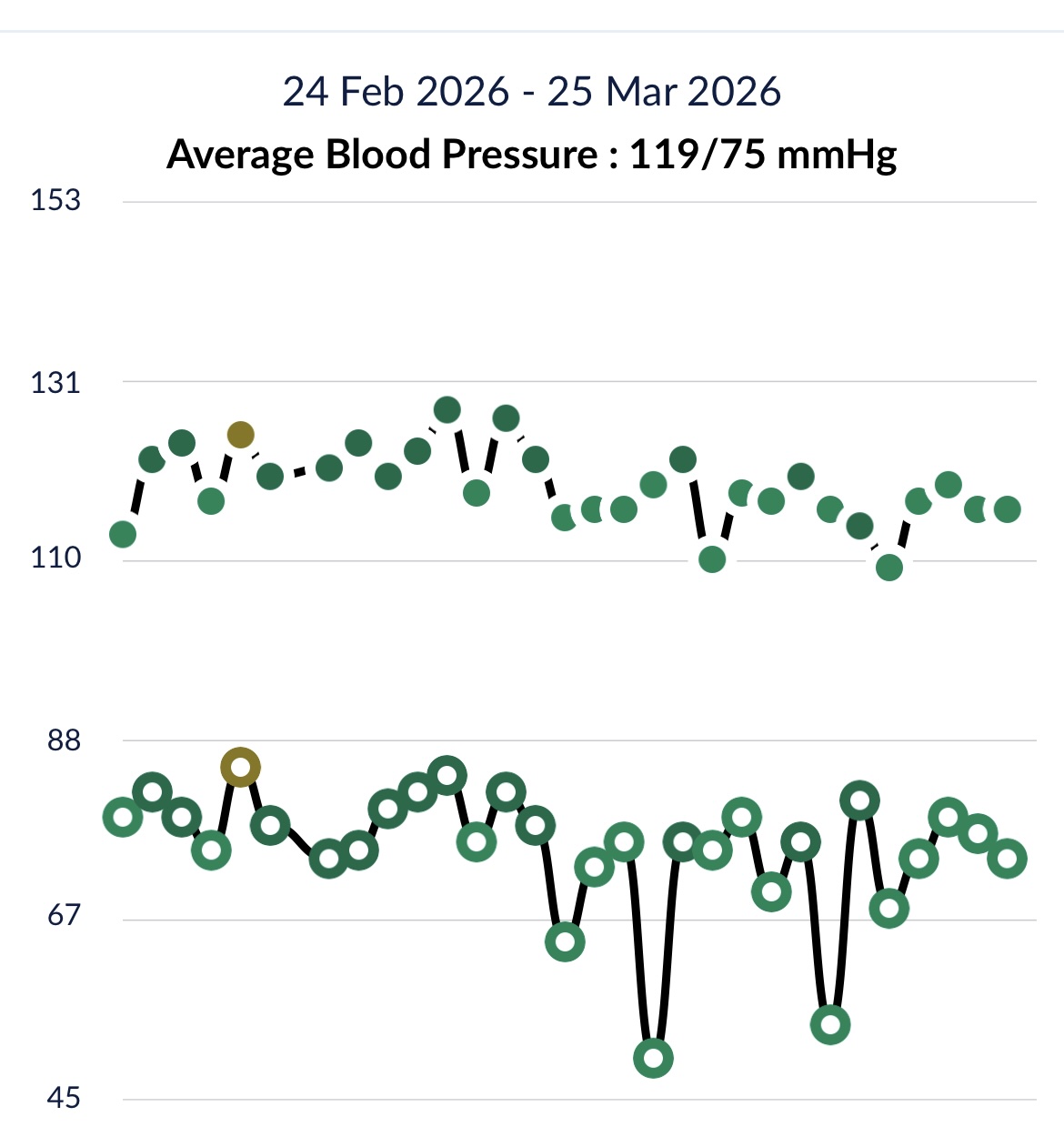
To make this a bit more real, below you can see my blood pressure readings over a month period:
Diet and lifestyle changes you can make.
Given how critical cardiovascular health is (recall it is the number one cause of death globally), then it is vital to adopt and maintain a lifestyle that maintains great heart health or seeks to address poor heart health. A number of the Big10 are aimed at maintaining and improving heart health and a wealth of information can be found in each of them. But, in summary:
Big10 #1: Avoid Ultra-Processed Foods and Control Your Insulin Levels
Big10 #2: Exercise Regularly and Include both Resistance and Cardiovascular Workouts
Big10 #3: Get Enough Good Quality Sleep
Big10 #5: Design Your Personal Supplement Stack Informed by Blood Testing
Big10 #9: Eat Healthily and Prioritise Building a Strong Gut Microbiome
Heart health scans
Along with monitoring your blood pressure, another valuable source of data can be obtaining a scan of your heart to look specifically for the buildup of plaque. In this section we look at two specific scans:
- A Coronary Calcium (CT) Scan
- A CT Coronary Angiogram (CTCA)
What is a Coronary Calcium (CT) Scan?
A coronary calcium CT (computed tomography) scan is a non-invasive scan that uses X-rays from many angles to build up a detailed 3D picture of (specifically in this case) the heart’s coronary arteries with the aim of detecting calcium buildup. It relies on calcium being a dense material that absorbs X-rays (similar to how bones are visualised). In essence, the term computed tomography means to take many flat images (slices) and then stack them to build a 3D image - much like the flat slices of a loaf of bread stack to create a 3D loaf of bread. The arteries that are of interest in the interpretation of this scan are the arteries that supply blood to the heart and enable it to do its work of pumping blood around the body.
Why should you care about coronary calcium scans?
The scan measures calcium deposits in the coronary arteries. Calcium deposits are an indicator of the amount of plaque built up in those arteries. Plaque is a mixture of fat and cholesterol that calcium sticks to, thus making it visible to the scan. This narrowing can sometimes lead to symptoms such as chest pain (angina), fatigue and shortness of breath. In the event of the plaque rupturing and a piece breaking off, this can lead to a blockage of the arteries and a sudden partial or total loss of blood supply to an area of the heart. This is commonly called a ‘heart attack’ or a Myocardial Infarction (MI). The proper term for the buildup of plaque and the hardening of the arteries is atherosclerosis. It may be inferred that if plaque can be detected within the arteries of the heart, then it may also be present in the carotid arteries (that supply the brain). The consequence of such plaque could be a stroke (caused either by the narrowing of arteries leading to the brain or a piece of the plaque breaking off/rupturing causing a clot which travels to the brain or blocks the artery).
To be a little more specific, there are three types of plaque:
- Non-calcified (soft) plaque
- Partially calcified (hardened) plaque
- Heavily calcified
Soft plaque is essentially a greater risk since it can easily be ruptured, leading to a clotting reaction due to the plaque contents spilling into the blood. This sudden clot (rather than the slowly building-up plaque) is what can lead to a heart attack. Harder plaque (which has been calcified by the body specifically to avoid this rupture risk) is more stable, and although it can narrow the artery (leading to chest pain), it would be less likely to cause a sudden heart attack.
We are using the level of calcium as a proxy for the plaque that might be present (it is not the calcium per-se that poses a risk, it is simply an indicator of plaque which poses the actual risk). The scan interpretation gives a score (where the lower the number, the lower the inferred buildup of plaque and thus a lower inferred risk of a heart attack in the coming years). An ideal score would be zero, indicating no observable calcium deposits/ plaque, but bear in mind that this is age-dependent and that a higher score may be expected for someone more elderly, whereas in a younger person it would be a cause for concern. Your score should be considered against your age, gender and family history.
Knowing your score enables your doctor or consultant to suggest lifestyle changes, medication, or more aggressive treatment depending on the severity of the condition that the score indicates.
Remember, this is only a scan of the arteries supplying the heart and does not directly measure the carotid arteries (those supplying the brain) thus it could be possible to have a zero score and yet still have plaque in the carotid arteries. A coronary calcium scan provides a specific view of the heart but only a general sense of plaque levels more widely.
There are some limitations of a coronoary calcium scan
- It cannot provide any information on soft/ non-calcified plaques, meaning that a score of zero cannot be used to rule out coronary artery disease.
- For non-zero scores it cannot provide a measure of the level of obstruction or narrowing (stenosis) of the arteries.
- Due to differences in evaluation techniques, the comparison of different measurements over time may not be reliable.
- It is possible that a rising score across serial tests may actually indicate an improvement in the underlying risk as softer plaque is encouraged to calcify (harden) due to a treatment programme (e.g. an intensive course of statins). [2]
Unlike a coronary calcium scan, which can only detect hardened plaque, a CT Coronary Angiogram (CTCA) scan can detect both hard and soft plaque and may also be able to provide a view of the impact on blood flow. However, this scan is a little more involved than a Coronary Calcium scan since it does require the intravenous introduction of a contrast dye into your body to make the arteries visible. For this reason, a coronary angiogram is normally used when there’s a clear reason to investigate. Whereas the slighty less invasive coronary calcium scan may be more appropriate for otherwise healthy people who want a ‘check-up’ of their heart. You can think of the CT calcium as a general screening test, whereas a coronary angiogram is a more detailed investigation. It’s important to discuss with your doctor (given your own health history) which scan would be most appropriate for you.
How much does a Coronary Calcium scan cost?
Unless referred by your doctor due to a specific concern, you will likely need to pay for this privately. For the scan along with interpretation and a consultation, you would expect to pay around £500 (convert this…).
I booked mine through Scan.com, had the scan conducted at Virtual Cath Lab (VCL) Surrey and was very satisfied with the service, the consulation, and the report (along with access to my scan images) that was provided. But, of course, you should have a look around as a number of providers are available.
What did I learn from my Coronary Calcium Scan?
The headline of my report was:
“The calcium score is zero. No aortic valve calcification. Limited images of the lungs, mediastinum, upper abdomen and bones are unremarkable.”
This was a reassuring result and provided positive feedback for the heart-healthy lifestyle I lead and choices I make. However, given my genetic pre-disposition for Lp(a) and the fact that I had levels of apoB and Triglycerides both above normal before taking action (along with a suboptimal Omega-6: Omega-3 ratio), I will likely also organise a CTCA scan to look for evidence of soft plaque.
Further sources of information
The Examine web site for independent, unsponsored meta-analyses of health research
Dr Pradip Jamnadas on the Diary of a CEO podcast
References
[1] World Health Organization (2021). “Cardiovascular diseases (CVDs) Fact Sheet.” WHO Newsroom.
[2] Puri, R., et al. (2015). “Impact of statins on serial coronary calcification during atheroma progression and regression.” Journal of the American College of Cardiology.